
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to 2009 oite review
Similar to 2009 oite review (20)
Recently uploaded
Recently uploaded (20)
2009 oite review
- 1. Question #: 1 Which of the following structures represents a site of compression of the median nerve at the elbow? 1- Ligament of Struthers 2- Intermuscular septum 3- Osborne’s ligament 4- Fascia of the flexor carpi ulnaris 5- Flexor-pronator aponeurosis in the forearm Preferred Response: 1 Recommended Reading(s): Elhassan B, Steinmann SP: Entrapment neuropathy of the ulnar nerve. J Am Acad Orthop Surg 2007;15:672-681. Bainbridge C: Cubital tunnel syndrome, in Berger RA, Weiss APC (eds): Hand Surgery. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 887-896. Question #: 2 In infants with congenital muscular torticollis, passive stretching exercises should include 1- lateral head tilt with no rotation. 2- lateral head tilt and chin rotation toward the affected side. 3- lateral head tilt and chin rotation away from the affected side. 4- lateral head tilt toward the affected side and chin rotation away from the affected side. 5- lateral head tilt away from the affected side and chin rotation toward the affected side. Preferred Response: 5 Recommended Reading(s): Coventry MB, Harris LE: Congenital muscular torticollis in infancy: Some observations regarding treatment. J Bone Joint Surg Am 1959;41:815-822. Loder RT: The cervical spine, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, pp 871-919.
- 2. Question #: 3 What is the best way to prevent failure due to cut-out after fixation of an unstable four-part intertrochanteric fracture with a compression hip screw device? 1- Use of an extra large screw and deep thread design 2- Use of a supplemental anti-rotation screw 3- A Dimon-Hughston medialization to allow load sharing 4- Screw tip placement in the inferior hemisphere of the femoral head 5- Screw tip placement with a tip-apex distance of less than 25 mm Preferred Response: 5 Recommended Reading(s): Baumgaertner MR, Curtin SL, Lindskog DM, et al: The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am 1995;77:1058-1064. Kyle RF, Gustilo RB, Premer RF: Analysis of six hundred and twenty-two intertrochanteric hip fractures. J Bone Joint Surg Am 1979;61:216-221. Koval KJ, Zuckerman JD: Intertrochanteric fractures, in Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 1635-1663. Question #: 4 Cuboidal cells that line along layers of immature osteoid to synthesize bone matrix and are not directly inhibited by bisphosphonates are best described as 1- osteoblasts. 2- osteocytes. 3- osteoclasts. 4- histiocytes. 5- megakarocytes. Preferred Response: 1 Recommended Reading(s): Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 189-196. Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 129-159.
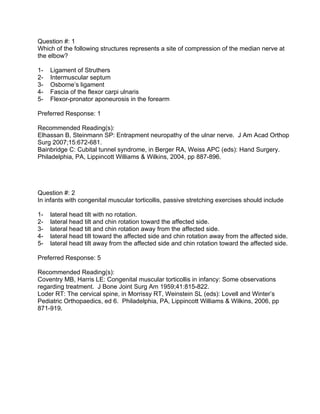
- 3. Figure 5a Figure 5b Question #: 5 Figures 5a and 5b show the radiographs of a 64-year-old man who underwent primary total hip arthroplasty 3 months ago for degenerative arthritis. He has now had four dislocations. How should his instability be managed? 1- Acetabular revision 2- Femoral head revision 3- Femoral head and stem revision 4- Abduction orthosis for 6 weeks 5- Placement of a constrained acetabular liner Preferred Response: 1 Recommended Reading(s): Dorr LD, Wan Z: Causes of and treatment protocol for instability of total hip replacement. Clin Orthop Relat Res 1998;355:144-151. Morrey BF: Instability after total hip arthroplasty. Orthop Clin North Am 1992;23:237-248.
- 4. Figure 6 Question #: 6 A 44-year-old woman undergoes a CT myelogram for evaluation of persistent low back pain and bilateral lower extremity paresthesias. Axial imaging through the vertebral body of L4 is shown in Figure 6. Further management should include which of the following? 1- Nuclear bone scan 2- Serum immunoelectrophoresis 3- Biopsy of lytic lesions of the vertebral body 4- Continued observation of the patient’s clinical course 5- Serum thyroid studies Preferred Response: 4 Recommended Reading(s): Ross JS, Bell GR: Spine imaging, in Herkowitz HN, Garfin SR, Eismont FJ, et al (eds): Rothman-Simeone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 187- 217.
- 5. Question #: 7 Which of the following physical examination findings is most helpful to diagnose a fixed posterior shoulder dislocation? 1- Apprehension sign 2- Sulcus sign 3- Jerk test 4- Jobe relocation test 5- Lack of external rotation Preferred Response: 5 Recommended Reading(s): Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 301-311. Ivkovic A, Boric I, Cicak N: One-stage operation for locked bilateral posterior dislocation of the shoulder. J Bone Joint Surg Br 2007;89:825-828.
- 6. Figure 8 Question #: 8 Figure 8 shows the radiograph of a 14-year-old girl with sickle cell disease and mild left hip discomfort. What is the radiographic natural history of this disease process? 1- Initial loss of sphericity of the femoral head with later restoration of sphericity 2- Maintenance of sphericity of the femoral head 3- Coxa magna without loss of sphericity of the femoral head 4- Progressive loss of sphericity of the femoral head 5- Protrusio acetabuli Preferred Response: 4 Recommended Reading(s): Hernigou P, Habibi A, Bachir D, et al: The natural history of asymptomatic osteonecrosis of the femoral head in adults with sickle cell disease. J Bone Joint Surg Am 2006;88:2565- 2572. Aguilar C, Vichinsky E, Neumayr L: Bone and joint disease in sickle cell disease. Hematol Oncol Clin North Am 2005;19:929-941.
- 7. Question #: 9 In a reverse shoulder arthroplasty, placement of the glenoid component in a high position on the native glenoid places the patient at risk of 1- an acromial fracture. 2- scapular notching. 3- postoperative instability. 4- restricted external rotation. 5- early loss of glenoid fixation. Preferred Response: 2 Recommended Reading(s): Simovitch RW, Zumstein MA, Lohri E, et al: Predictors of scapular notching in patients managed with the Delta III reverse total shoulder replacement. J Bone Joint Surg Am 2007;89:588-600. Gutiérrez S, Levy JC, Lee WE III, et al: Center of rotation affects abduction range of motion of reverse shoulder arthroplasty. Clin Orthop Relat Res 2007;458:78-82. Question #: 10 Achondroplasia is associated with which of the following mutations? 1- Insulin-like growth factor-1 receptor 2- Insulin-like growth factor-1 3- Insulin-like growth factor-2 4- Fibroblast growth factor receptor-3 5- Fibroblast growth factor Preferred Response: 4 Recommended Reading(s): Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 3-23. Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 773-783.
- 8. Figure 11a Figure 11b Question #: 11 An otherwise healthy 20-year-old dancer has a 1-year history of foot and ankle pain. She describes her great toe locking with active range of motion. Examination reveals triggering of the great toe but no tenderness at the level of the first metatarsal head. Palpable crepitus is present along the medial ankle with active range of motion of the great toe. Radiographs are unremarkable. MRI scans are shown in Figures 11a and 11b. What is the most likely diagnosis? 1- Tarsal tunnel syndrome 2- Medial sesamoid stress fracture 3- Flexor hallucis longus tendon tear at the metatarsophalangeal joint 4- Flexor hallucis longus tendon tear at the posteromedial ankle 5- Chronic deep space infection of the posterior ankle Preferred Response: 4 Recommended Reading(s): Hamilton WG, Hamilton LH: Foot and ankle injuries in dancers, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1225-1256. Sammarco GJ, Cooper PS: Flexor hallucis longus tendon injury in dancers and nondancers. Foot Ankle Int 1998;9:356-362.
- 9. Question #: 12 A 15-year-old boy has diffuse back pain, particularly in the morning. Examination reveals an increased kyphosis in the thoracic spine. Spinal mobility in flexion and extension is limited. He has decreased chest excursion with inspiration. The FABER test is positive. Standing radiographs show absence of the anterior concavity of the vertebral body and a kyphosis of 62° from T-3 to T-12. What is the most likely diagnosis? 1- Pott disease 2- Reiter syndrome 3- Scheuermann’s kyphosis 4- Ankylosing spondylitis 5- Diffuse idiopathic skeletal hyperostosis Preferred Response: 4 Recommended Reading(s): Azouz EM, Dufy CM: Juvenile spondyloarthropathies: Clinical manifestations and medical imaging. Skeletal Radiol 1995;24:399-408. Gensler L, Davis JC Jr: Recognition and treatment of juvenile-onset spondyloarthritis. Curr Opin Rheumatol 2006;18:507-511. Kredich D, Patrone NA: Pediatric spondyloarthropathies. Clin Orthop Relat Res 1990;259:18-22. Question #: 13 Which of the following represents a contraindication to hyperbaric oxygen therapy? 1- Intubation 2- Osteomyelitis 3- Insulin pump 4- Thermal burns 5- Thoracostomy tube Preferred Response: 3 Recommended Reading(s): Greensmith JE: Hyperbaric oxygen therapy in extremity trauma. J Am Acad Orthop Surg 2004;12:376-384. Kindwall EP: Contraindications and side effects to hyperbaric oxygen treatment, in Kindwall EP, Whelan HT (eds): Hyperbaric medicine practice, ed 2. Flagstaff, AZ, Best Publishing Company, 1999, pp 83-98. Buettner MF, Wolkenhauer D: Hyperbaric oxygen therapy in the treatment of open fractures and crush injuries. Emerg Med Clin North Am 2007;25:177-188.
- 10. Question #: 14 A 42-year-old woman injured her dominant middle finger in a car door. Examination reveals a partial nail avulsion with nail bed lacerations. No fractures are seen on radiographs. Without compromising functional and cosmetic results, what is the most expeditious treatment? 1- Placement of 6-0 chromic suture 2- Placement of 6-0 fast-absorbing gut suture 3- Application of a saline gauze dressing 4- Application of a non-adherent dressing 5- Application of 2-octylcyanoacrylate Preferred Response: 5 Recommended Reading(s): Strauss EJ, Weil WM, Jordan C, et al: A prospective, randomized, controlled trial of 2- octylcyanoacrylate versus suture repair for nail bed injuries. J Hand Surg Am 2008;33:250- 253. Richards AM, Chrick A, Cole RP: A novel method of securing the nail following nail bed repair. Plast Reconstr Surg 1999;103:1983-1985.
- 11. Figure 15a Figure 15b Question #: 15 Figures 15a and 15b show the bone scan and CT scan of a 20-year-old collegiate football player who has persistent low back pain without neurologic symptoms. What physical examination maneuver would you expect to be abnormal? 1- Babinski test 2- Femoral stretch test 3- Straight leg raise 4- Contralateral straight leg raise 5- Single-limb standing lumbar extension Preferred Response: 5 Recommended Reading(s): Hu SS, Tribus CB, Diab M, et al: Spondylolisthesis and spondylolysis. J Bone Joint Surg Am 2008;90:656-671. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont IL, American Academy of Orthopaedic Surgeons, 2004, pp 19-28.
- 12. Question #: 16 During surgical reduction of a congenitally dislocated hip through an anteromedial approach, what structure is most at risk when performing the psoas tenotomy? 1- Femoral vein 2- Femoral artery 3- Lateral circumflex artery 4- Medial circumflex artery 5- Obturator artery Preferred Response: 4 Recommended Reading(s): Morrissy RT, Weinstein SL: Atlas of Pediatric Orthopaedic Surgery, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, pp 271-277. Weinstein SL, Ponseti IV: Congenital dislocation of the hip. J Bone Joint Surg Am 1979;61:119-124.
- 13. Figure 17a Figure 17b Figure 17c Figure 17d
- 14. Question #: 17 The 20-year-old man sustains the fracture seen in Figures 17a through 17d. What technical aspect of the surgical treatment is most important for the patient’s outcome? 1- Restoring fibular length 2- Achieving fibular compression 3- Reduction of the posterior malleolus 4- Reduction of the anteromedial impacted fragments 5- Fixing the distal tibiofibular syndesmosis Preferred Response: 4 Recommended Reading(s): Marsh JL, Saltzman CL: Ankle fractures, in Rockwood and Green’s Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, pp 2147-2247. McConnell T, Tornetta P III: Marginal plafond impaction in association with supination- adduction ankle fractures: A report of eight cases. J Orthop Trauma 2001;15:447-449. Question #: 18 A unicompartment knee arthroplasty is contraindicated in which of the following clinical scenarios? 1- Inflammatory arthritis 2- Anteromedial osteoarthritis 3- Lateral compartment osteoarthritis 4- Medial femoral condyle osteonecrosis 5- Advanced age Preferred Response: 1 Recommended Reading(s): Marmor L: Unicompartment arthroplasty for osteonecrosis of the knee joint. Clin Orthop Relat Res 1993;294:247-253. Parrette S, Argenson JN, Dumas J, et al: Unicompartmental knee arthroplasty for avascular necrosis. Clin Orthop Relat Res 2007;464:37-42. Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 457-471.
- 15. Question #: 19 Decreased stature and bone density due to lead poisoning is thought to be caused by interference in the signaling of which of the following growth factors? 1- BMP2 2- RANKL 3- PTHrP/TGF-beta 4- Fibroblast growth factor 3 (FGF3) 5- Insulin-like growth factor (IGF) Preferred Response: 3 Recommended Reading(s): Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 115-127. Campbell JR, Rosier RN, Novotny L, et al: The association between environmental lead exposure and bone density in children. Environ Health Perspect 2004;112:1200-1203. Question #: 20 Which of the following is considered the strongest predictor of disability in adult patients with scoliosis? 1- Concomitant diagnosis of osteoporosis 2- Presence of a vacuum disk sign at two or more lumbar levels 3- Sagittal plane imbalance and inability to obtain neutral upright stance 4- The number of spinal levels affected by disk degeneration in the lumbar spine 5- Coronal plane Cobb angle measurement of greater than 30° in the lumbar spine Preferred Response: 3 Recommended Reading(s): Schwab F, Farcy JP, Bridwell K, et al: A clinical impact classification of scoliosis in the adult. Spine 2006;31:2109-2114. Glassman SD, Bridwell K, Dimar JR, et al: The impact of positive sagittal balance in adult spinal deformity. Spine 2005;30:2024-2029. Kim YJ, Bridwell KH, Lenke LG, et al: Sagittal thoracic decompensation following long adult lumbar spinal instrumentation and fusion to L5 or S1: Causes, prevalence, and risk factor analysis. Spine 2006;31:2359-2366.
- 16. Figure 21a Figure 21b Question #: 21 A 9-year-old boy is seen for bilateral thigh pain. He has a history of precocious puberty. Examination reveals multiple café-au-lait spots. AP pelvis and frog lateral hip radiographs are shown in Figures 21a and 21b. His condition is linked to an abnormality in 1- G protein function. 2- osteoclastic function. 3- vitamin D metabolism. 4- sulfate transporter gene. 5- type I collagen formation. Preferred Response: 1 Recommended Reading(s): DiCaprio MR, Enneking WF: Fibrous dysplasia: Pathophysiology, evaluation, and treatment. J Bone Joint Surg Am 2005;87:1848-1864. Parekh SG, Donthineni-Rao R, Ricchetti E, et al: Fibrous dysplasia. J Am Acad Orthop Surg 2004;12:305-313.
- 17. Question #: 22 What is the incidence of full-thickness rotator cuff tears in patients undergoing arthroplasty for the treatment of primary glenohumeral osteoarthritis? 1- 1% to 2% 2- 5% to 10% 3- 10% to 15% 4- 15% to 20% 5- 20% to 25% Preferred Response: 2 Recommended Reading(s): Edwards TB, Boulahia A, Kempf JF, et al: The influence of rotator cuff disease on the results of shoulder arthroplasty for primary osteoarthritis: Results of a multicenter study. J Bone Joint Surg Am 2002;84:2240-2248. Norris TR, Iannotti JP: Functional outcome after shoulder arthroplasty for primary osteoarthritis: A multicenter study. J Shoulder Elbow Surg 2002;11:130-135. Question #: 23 In children with Morquio syndrome, atlantoaxial instability is most commonly the result of 1- hypoplasia of the odontoid. 2- failure of fusion of the base of the odontoid. 3- incompetence of the transverse ligament. 4- generalized joint hypermobility. 5- erosion of the odontoid base due to synovial hypertrophy. Preferred Response: 1 Recommended Reading(s): Copley LA, Dormans JP: Cervical spine disorders in infants and children. J Am Acad Orthop Surg 1998;6:204-214. Stevens JM, Kendall BE, Crockard HA: The odontoid process in Morquio-Brailsford’s disease: The effects of occipitocervical fusion. J Bone Joint Surg Br 1991;73:851-858.
- 18. Question #: 24 A 51-year-old woman has had left hand numbness for the past 2 years. Examination reveals decreased sensation over the fifth metacarpal region and little finger, both palmar and dorsal. There is no loss of abduction/adduction strength. Brace treatment has failed to provide relief, and neurodiagnostic studies reveal ulnar nerve compression with increased latency. The next step in treatment is ulnar nerve decompression at the 1- wrist only. 2- wrist and the elbow without transposition. 3- wrist and the elbow with anterior submuscular transposition. 4- elbow only without transposition. 5- elbow only with anterior submuscular transposition. Preferred Response: 4 Recommended Reading(s): Zlowodzki M, Chan S, Bhandari M, et al: Anterior transposition compared with simple decompression for treatment of cubital tunnel syndrome: A meta-analysis of randomized, controlled trials. J Bone Joint Surg Am 2007;89:2591-2598. Bartels RH, Verhagen WI, van der Wilt GJ, et al: Prospective randomized controlled study comparing simple decompression versus anterior subcutaneous transposition for idiopathic neuropathy of the ulnar nerve at the elbow: Part 1. Neurosurgery 2005;56:522-530. Nabhan A, Ahlhelm F, Kelm J, et al: Simple decompression or subcutaneous anterior transposition of the ulnar nerve for cubital tunnel syndrome. J Hand Surg Br 2005;30:521- 524. Question #: 25 During the Henry (volar) approach for a junction mid and upper third diaphyseal radial shaft fracture, what nerve is most at risk for injury? 1- Ulnar 2- Radial 3- Median 4- Anterior interosseous 5- Posterior interosseous Preferred Response: 5 Recommended Reading(s): Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 1984, pp 58-63. Martini FH, Timmons MJ, Tallitsch RB: Human Anatomy, ed 5. San Francisco, CA, Pearson/Benjamin Cummings, 2006, pp 197-199.
- 19. Question #: 26 What is the most common reason for failure of anterior cruciate ligament reconstruction? 1- Malposition of the bone tunnels 2- Medial meniscus deficiency 3- Lateral meniscus deficiency 4- Improper graft selection 5- Articular surface damage Preferred Response: 1 Recommended Reading(s): Battaglia TC, Miller MD: Management of bony deficiency in revision anterior cruciate ligament reconstruction using allograft bone dowels: Surgical technique. Arthroscopy 2005;21:767. Grossman MG, ElAttrache NS, Shields CL, et al: Revision anterior cruciate ligament reconstruction: Three- to nine-year follow-up. Arthroscopy 2005;21:418-423.
- 20. Figure 27a Figure 27b Question #: 27 A 75-year-old woman has a slow growing mass in her thigh. She reports difficulty walking because of the increasing size of the mass. Chest imaging shows no evidence of metastatic disease. A radiograph and a T1-weighted MRI scan are shown in Figures 27a and 27b. What is the next step in management? 1- Biopsy 2- Surgical excision 3- Preoperative radiation therapy 4- Preoperative chemotherapy 5- Treatment with pain medication, physical therapy, and follow-up in 12 months Preferred Response: 2 Recommended Reading(s): Schwartz HS (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 277-287. Dalal KM, Antonescu CR, Singer S: Diagnosis and management of lipomatous tumors. J Surg Oncol 2008;97:298-313.
- 21. Question #: 28 A patient who underwent intramedullary nailing of a femoral shaft fracture 2 weeks ago now reports hip pain that radiates to the knee. What is the next most appropriate step in management? 1- Reassure the patient that the pain will improve and order physical therapy. 2- Review the radiographic report from the time of injury. 3- Obtain an AP and lateral view of the hip. 4- Obtain an MRI of the lumbar spine. 5- Obtain lumbar spine radiographs. Preferred Response: 3 Recommended Reading(s): Tornetta P III, Kain MS, Creevy WR: Diagnosis of femoral neck fractures in patients with a femoral shaft fracture: Improvement with a standard protocol. J Bone Joint Surg Am 2007;89:39-43. Daffner RH, Riemer BL, Butterfield SL: Ipsilateral femoral neck and shaft fractures: An overlooked association. Skeletal Radiol 1991;20:251-254.
- 22. Figure 29a Figure 29b Figure 29c
- 23. Question #: 29 A 2½-year-old boy is examined for flat feet. Examination reveals bilateral flat feet, with the left side affected more than the right. The arch on his right foot is restored when he stands on his toes or is sitting. The left foot remains flat when standing on his toes or sitting. AP, lateral, and plantar flexion lateral radiographs of the left foot are shown in Figures 29a through 29c. Treatment of the left foot should consist of 1- triple arthrodesis. 2- serial casting followed by application of a foot abduction orthosis. 3- a supramalleolar orthosis. 4- surgical correction of the midfoot and heel cord lengthening. 5- talectomy. Preferred Response: 4 Recommended Reading(s): Sullivan JA: Pediatric flatfoot: Evaluation and management. J Am Acad Orthop Surg 1999;7:44-53. Drennan JC: Congenital vertical talus. Instr Course Lect 1996;45:315-322.
- 24. Figure 30 Question #: 30 What anatomic structure is at the tip of the arrow in Figure 30? 1- Anterior sacral artery 2- S1 nerve root 3- L5 nerve root 4- Iliac vein 5- Sympathetic chain Preferred Response: 3 Recommended Reading(s): Louis R: Fusion of the lumbar and sacral spine by internal fixation with screw plates. Clin Orthop Relat Res 1986;203:18-33. Aylwin A, Saifuddin A, Tucker S: L5 radiculopathy due to sacral stress fracture. Skeletal Radiol 2003;32:590-593.
- 25. Figure 31a Figure 31b Figure 31c
- 26. Question #: 31 A 48-year-old woman fell onto her outstretched arm 8 weeks ago. Radiographs at the time of injury revealed a comminuted radial head fracture and no dislocation. She was initially treated with early mobilization. Examination reveals no medial-sided tenderness or bruising and no wrist pain. She has a persistent block to supination and extension. CT scans are shown in Figures 31a through 31c. Treatment at this time should consist of 1- radial head arthroplasty. 2- resection of the radial head. 3- open reduction and internal fixation of the radial head. 4- manipulation under anesthesia with an intra-articular steroid injection. 5- arthroscopic debridement of the elbow. Preferred Response: 2 Recommended Reading(s): Herbertsson P, Josefsson PO, Hasserius R, et al: Uncomplicated Mason type-II and III fractures of the radial head and neck in adults: A long-term follow-up study. J Bone Joint Surg Am 2004;86:569-574. Jackson JD, Steinmann SP: Radial head fractures. Hand Clin 2007;23:185-193.
- 27. Figure 32a Figure 32b Question #: 32 A 45-year-old man reports a 6-month history of lateral foot pain. Radiographs are shown in Figures 32a and 32b. What is the most appropriate orthotic device for this patient? 1- Solid ankle cushioned heel 2- Three-quarter length rigid insole with medial hindfoot and forefoot posting 3- Full-length rigid insole with medial forefoot posting 4- Full-length semi-rigid insole with medial hindfoot and forefoot posting 5- Full-length semi-rigid insole with a depression for the first ray and a lateral wedge Preferred Response: 5 Recommended Reading(s): Manoli A II, Graham B: The subtle cavus foot, “the underpronator.” Foot Ankle Int 2005;26:256-263. Janisse DJ, Janisse E: Shoe modification and the use of orthoses in the treatment of foot and ankle pathology. J Am Acad Orthop Surg 2008;16:152-158.
- 28. Figure 33 Question #: 33 Figure 33 shows the radiograph of an 84-year-old woman who is seen in the emergency department with new onset severe right groin pain and inability to bear weight. She does not recall a fall but uses a walker and frequently stumbles. Laboratory studies, including a CBC, erythrocyte sedimentation rate, and C-reactive protein, are all normal. What is the most likely diagnosis? 1- Septic total hip 2- Metastasis to pelvis 3- Insufficiency fracture of the ramus 4- Primary bony malignancy 5- Loose acetabular component Preferred Response: 3 Recommended Reading(s): Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 289-306. Vanderschot P: Treatment options of pelvic and acetabular fractures in patients with osteoporotic bone. Injury 2007;38:497-508.
- 29. Question #: 34 Randomized controlled trials are considered to provide the highest level of evidence, and concealed treatment allocation is essential to prevent bias in this study design. Concealment is best achieved by using 1- even-odd days. 2- patient birth date. 3- randomization by surgeon. 4- patient hospital identification number. 5- opaque envelopes containing the randomization number. Preferred Response: 5 Recommended Reading(s): Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 87-101. Poolman RW, Struijs PA, Krips R, et al: Reporting of outcomes in orthopaedic randomized trials: Does blinding of outcome assessors matter? J Bone Joint Surg Am 2007;89:550- 558. Question #: 35 A 25-year-old competitive soccer player has chronic anterior knee pain and reports “sloppiness” since injuring it in a collision with another player 2 months ago. He missed several weeks of practice but has since attempted a return to play. Examination reveals no quadriceps atrophy, standing varus alignment of 8°, a posterior sag sign, 3+ posterior drawer, 2+ varus instability in extension, 3+ varus instability at 30°, and 20° increased prone external rotation at 30° and 90°. He walks with a varus thrust. What is the best treatment option? 1- High tibial osteotomy 2- Reconstruction of the posterior cruciate ligament (PCL) and repair of the posterolateral corner (PLC) 3- Reconstruction of the PCL 4- Reconstruction of the PCL and PLC 5- High tibial osteotomy and PCL/PLC reconstruction Preferred Response: 5 Recommended Reading(s): Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 183-197. Giffin JR, Vogrin TM, Zantop T, et al: Effects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med 2004;32:376-382.
- 30. Question #: 36 When assessing the location of a guide pin for minimal-open screw fixation of a transverse scaphoid waist fracture, which of the following locations provides the best biomechanical fixation? 1- Central axis of the proximal and distal fragments 2- Dorsal axis in the distal and proximal fragments 3- Volar axis in the distal and proximal fragments 4- Dorsal axis distally and volar axis in the proximal fragment 5- Volar axis distally and dorsal axis in the proximal fragment Preferred Response: 1 Recommended Reading(s): McCallister WV, Knight J, Kaliappan R, et al: Central placement of the screw in simulated fractures of the scaphoid waist: A biomechanical study. J Bone Joint Surg Am 2003;85:72- 77. Dodds SD, Panjabi MM, Slade JF III: Screw fixation of scaphoid fractures: A biomechanical assessment of screw length and screw augmentation. J Hand Surg Am 2006;31:405-413. Question #: 37 What is the most frequent variant of the relationship between the sciatic nerve and the piriformis tendon as the nerve exits the sciatic notch? 1- Entire nerve courses anterior to the piriformis muscle 2- Entire nerve courses posterior to the piriformis muscle 3- Entire nerve pierces and divides the piriformis muscle 4- Nerve divides and courses around the piriformis muscle 5- Nerve divides, with one division dividing the piriformis muscle Preferred Response: 1 Recommended Reading(s): Pokorny D, Jahoda D, Veigl D, et al: Topographic variations of the relationship of the sciatic nerve and the piriformis muscle and its relevance to palsy after total hip arthroplasty. Surg Radiol Anat 2006;28:88-91. Tornetta P III: Hip dislocations and fractures of the femoral head, in Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, p 1556. Beaton LE, Anson BJ: The relation of the sciatic nerve and of its subdivisions to the piriformis muscle. Anat Rec 1937;70:1-5.
- 31. Figure 38a Figure 38b Figure 38c Figure 38d
- 32. Question #: 38 A 36-year-old woman has right knee pain and swelling that first began 4 months ago. Figures 38a through 38d show radiographs, MRI scans, and H & E histology slides at 20X and 100X. These findings are most consistent with what diagnosis? 1- High-grade central osteosarcoma 2- Periosteal osteosarcoma 3- Juxta-articular chondroma 4- Osteochondroma 5- Bizarre parosteal osteochondromatous proliferation (Nora’s lesion) Preferred Response: 2 Recommended Reading(s): Campanacci M: Periosteal osteosarcoma, in Campanacci M (ed): Bone and soft tissue tumors, ed 2. New York, NY, Springer-Verlag Wien, 1999, pp 517-524. Weis L: Common malignant bone tumors, in Simon M, Springfield D (eds): Osteosarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, pp 265-274.
- 33. Question #: 39 An 18-month-old boy is being evaluated for intoeing gait. Foot progression angles are -10°. Thigh-foot angles are -20° bilaterally. There is no metatarsus adductus. His height is in the 60th percentile for his age. What is the most appropriate treatment? 1- Observation 2- Denis Browne bar 3- Referral to physical therapy 4- Vitamin D, calcium, and phosphate levels 5- Bilateral knee-ankle-foot orthoses with a medial upright Preferred Response: 1 Recommended Reading(s): Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320. Staheli LT: Rotational problems in children. Instr Course Lect 1994;43:199-209. Kling TF Jr, Hensinger RN: Angular and torsional deformities of the lower limbs in children. Clin Orthop Relat Res 1983;176:136-147. Question #: 40 Postoperative loss of reduction after iliosacral screw fixation of a posterior pelvic ring injury has been attributed to which of the following? 1- Use of a partially threaded screw 2- Vertical fracture pattern through the sacrum 3- Lateral compression fracture pattern 4- Open book fracture pattern 5- Initial non-anatomic reduction Preferred Response: 2 Recommended Reading(s): Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 389-397. Griffin DR, Starr AJ, Reinert CM, et al: Vertically unstable pelvic fractures fixed with percutaneous iliosacral screws: Does posterior injury pattern predict fixation failure? J Orthop Trauma 2006;20:S30-S36.
- 34. Question #: 41 A 65-year-old man with a distal femoral low grade exostotic chondrosarcoma reports mild knee pain. Radiologic work-up reveals no metastases. The patient’s leg otherwise functions normally. Definitive treatment for this tumor consists of 1- wide excision only. 2- chemotherapy only. 3- chemotherapy followed by wide excision. 4- radiation therapy only. 5- radiation therapy followed by wide excision. Preferred Response: 1 Recommended Reading(s): Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 187-202. Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338. Question #: 42 Shoulder pathology in adult patients with juvenile idiopathic arthritis (formerly juvenile rheumatoid arthritis) is characterized by 1- above average bone density. 2- large bone size. 3- a superiorly migrated humeral head. 4- medialization of the humeral head due to glenoid bone loss. 5- significant posterior glenoid erosion. Preferred Response: 4 Recommended Reading(s): Thomas S, Price AJ, Sankey RA, et al: Shoulder hemiarthroplasty in patients with juvenile idiopathic arthritis. J Bone Joint Surg Br 2005;87:672-676. Jolles BM, Grosso P, Bogoch ER: Shoulder arthroplasty for patients with juvenile idiopathic arthritis. J Arthroplasty 2007;22:876-883.
- 35. Question #: 43 An acutely injured quadriplegic patient undergoes an anterior diskectomy and fusion with plating at C6-7. Two days postoperatively the patient has sweating, a severe headache, flushing, and a blood pressure of 180/120 mm Hg. What is the most appropriate initial management? 1- IV administration of epinephrine 2- MRI of the cervical spine 3- Removal of the cervical plate 4- Irrigation and/or replacement of the indwelling urinary catheter 5- Placement of a lumbar subarachnoid drain Preferred Response: 4 Recommended Reading(s): Banovac K, Sherman AL: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Eismont FJ, et al (eds): Rothman-Simeone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1220-1231. Furlan JC, Fehlings MG: Cardiovascular complications after acute spinal cord injury: Pathophysiology, diagnosis, and managment. Neurosurg Focus 2008;25:E13.
- 36. Figure 44a Figure 44b Question #: 44 The clinical test shown in Figures 44a and 44b, in which the hip is first flexed, abducted, and externally rotated, and then is extended and allowed to fall into adduction and internal rotation, tests for contractures of what muscle? 1- Sartorius 2- Pectineus 3- Gluteus medius 4- Rectus femoris 5- Tensor fascia lata Preferred Response: 5 Recommended Reading(s): Herring JA: The orthopaedic examination: A comprehensive overview, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 27-53. Gross R: Physical examination, in Staheli LT (ed): Pediatric Orthopaedic Secrets, ed 2. Philadelphia, PA, Hanley Belfus, 2003, p 15.
- 37. Question #: 45 In synovial fluid analysis before revision total knee arthroplasty, what is the minimum threshold for white blood cell count that is considered strongly indicative of infection? 1- 100 2- 500 3- 2,500 4- 10,000 5- 25,000 Preferred Response: 3 Recommended Reading(s): Mason JB, Fehring TK, Odum SM, et al: The value of white blood cell counts before revision total knee arthroplasty. J Arthroplasty 2003;18:1038-1043. Parvizi J, Ghanem E, Menashe S, et al: Periprosthetic infection: What are the diagnostic challenges? J Bone Joint Surg Am 2006;88:138-147. Schinsky MF, Della Valle CJ, Sporer SM, et al: Perioperative testing for joint infection in patients undergoing revision total hip arthroplasty. J Bone Joint Surg Am 2008;90:1869- 1875. Question #: 46 A patient has a both bone forearm fracture. After open reduction and internal fixation with modern plating techniques, addition of a bone graft to the radius is indicated if there is which of the following findings? 1- Forty percent comminution of the circumference of the radius 2- Segmental fracture of the ulna 3- Segmental bone loss of the radius 4- Open radius and ulna fractures 5- Open radius fracture Preferred Response: 3 Recommended Reading(s): Wright RR, Schmeling GJ, Schwab JP: The necessity of acute bone grafting in diaphyseal forearm fractures: A retrospective review. J Orthop Trauma 1997;11:288-294. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 307-316. Moed BR, Kellam JF, Foster RJ, et al: Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am 1986;68:1008-1017.
- 38. Question #: 47 Which of the following modes better defines corrosion resulting from an electrochemical potential created between two metals in contact and immersed in a conductive medium? 1- Crevice 2- Galvanic 3- Fretting 4- Degradation 5- Delamination Preferred Response: 2 Recommended Reading(s): Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 65-85. Mazzocca AD, Caputo AE, Browner BD, et al: Principles of internal fixation, in Browner BD, Jupiter JB, Levine AM (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 195-249.
- 39. Figure 48 Question #: 48 A 4-year-old boy injures his finger in a lawn mower. A clinical photograph of the palmar side of the little finger is shown in Figure 48. With exam under sedation, the bone is noted to be covered by the subcutaneous tissue. To preserve length, contour, and sensation, treatment after irrigation and debridement should consist of 1- a thenar flap. 2- a V-Y advancement flap. 3- direct closure. 4- microvascular reattachment. 5- application of antibiotic ointment and a sterile dressing. Preferred Response: 5 Recommended Reading(s): Lamon RP, Cicero JJ, Frascone RJ, et al: Open treatment of fingertip amputations. Ann Emerg Med 1983;12:358-360. Söderberg T, Nyström A, Hallmans G, et al: Treatment of fingertip amputations with bone exposure: A comparative study between surgical and conservative treatment methods. Scand J Plast Reconstr Surg 1983;17:147-152. Farrell RG, Disher WA, Nesland RS, et al: Conservative management of fingertip amputations. JACEP 1977;6:243-246.
- 40. Figure 49 Question #: 49 A 2-month-old boy is evaluated for short stature and severe clubfeet. Examination reveals swelling of the pinnae of the ears. The appearance of the hands and feet are shown in Figure 49. What is the most likely diagnosis? 1- Achondroplasia 2- Apert syndrome 3- Congenital syphilis 4- Diastrophic dysplasia 5- Cleidocranial dysplasia Preferred Response: 4 Recommended Reading(s): Sponseller PD: The skeletal dysplasias, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 243-285. Ryoppy S, Poussa M, Morikanto J, et al: Foot deformities in diastrophic dysplasia: An analysis of 102 patients. J Bone Joint Surg Br 1992;74:441-444.
- 41. Figure 50a Figure 50b Figure 50c Figure 50d
- 42. Question #: 50 A 34-year-old woman reports pain in the tibia. Radiographs, a CT scan, and a biopsy specimen are shown in Figures 50a through 50d. What is the most appropriate treatment option? 1- Observation 2- External beam radiation 3- Radiofrequency ablation 4- Curettage with power burr and packing with cement 5- Wide resection and osteoarticular allograft reconstruction Preferred Response: 4 Recommended Reading(s): Turcotte RE: Giant cell tumor of bone. Orthop Clin North Am 2006;37:35-51. Bini SA, Gill K, Johnston JO, et al: Giant cell tumor of bone: Curettage and cement reconstruction. Clin Orthop Relat Res 1995;321:245-250. Question #: 51 A 63-year-old man with a history of renal cell carcinoma has had severe thoracic pain for the past month. Examination shows mild lower extremity weakness with positive Babinski. Radiographs show a lytic lesion within T9 and a localized gibbus deformity of 40° from T8- T10. What is the most appropriate management prior to surgery? 1- Radiation therapy 2- Chemotherapy 3- Chemotherapy and radiation therapy 4- Epidural corticosteroid placement 5- Intra-arterial embolization Preferred Response: 5 Recommended Reading(s): Prabhu VC, Bilsky MH, Jambhekar K, et al: Results of preoperative embolization for metastatic spinal neoplasms. J Neurosurg 2003;98:156-164. Heary RF, Bono CM: Metastatic spinal tumors. Neurosurg Focus 2001;11:e1.
- 43. Question #: 52 In which of the following fracture patterns is the optimal orientation of the screws used to repair the medial malleolar fragment, parallel to the ankle joint? 1- Supination external rotation 2- Supination internal rotation 3- Pronation external rotation 4- Supination adduction 5- Pronation abduction Preferred Response: 4 Recommended Reading(s): Michelson JD: Ankle fractures resulting from rotational injuries. J Am Acad Orthop Surg 2003;11:403-412. Hak DJ, Lee MA: Ankle fractures: Open reduction internal fixation, in Wiss DA (ed): Master Techniques in Orthopaedic Surgery: Fractures, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, pp 551-567. Question #: 53 A 9-year-old boy with an L-4 level myelomeningocele is scheduled to undergo soft-tissue surgery for equinocavovarus feet. In addition to shunt clearance, what safety precautions should be taken in the perioperative period? 1- Latex-free environment 2- Avoidance of fiberglass casting material 3- Avoidance of intravenous narcotics 4- Hyperthermia prophylaxis 5- Preoperative echocardiogram Preferred Response: 1 Recommended Reading(s): Drennan JC: Current concepts in myelomeningocoele. Instr Course Lect 1999;48:543-550. Herring JA: Disorders of the spinal cord, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 1405-1482.
- 44. Figure 54a Figure 54b Question #: 54 A 7-month-old infant has the findings shown in Figures 54a and 54b. Which of the following approaches to the surgical reconstruction is most appropriate? 1- The intrinsic tendon and collateral ligament insertions from the radial thumb should be preserved. 2- The ulnar thumb should be deleted with transfer of the extensor tendons. 3- The radial half of one thumb should be combined with the ulnar half of the other to create one thumb (Bilhaut-Cloquet procedure). 4- The radial digital nerves should be transferred into the ulnar thumb. 5- Brunner incisions across the palmar surfaces should be avoided. Preferred Response: 1 Recommended Reading(s): Ogino T, Ishii S, Takahata S, et al: Long-term results of surgical treatment of thumb polydactyly. J Hand Surg Am 1996;21:478-486. Baek GH, Gong HS, Chung MS, et al: Modified Bilhaut-Cloquet procedure for Wassel type- II and III polydactyly of the thumb. J Bone Joint Surg Am 2007;89:534-541.
- 45. Question #: 55 Somitization of the axial skeleton has been shown to be highly dependent on what mechanism? 1- Sequential activation of homeobox genes 2- Notochord activation of sonic hedgehog 3- Formation of collagen 1 matrix in the ribosome 4- Dorsal sclerotome activation of MSX1 and MSX2 5- Alternation of activation of noggin and bone morphogenic proteins Preferred Response: 1 Recommended Reading(s): Iimura T, Pourquie PO: Hox genes in time and space during vertebrate body formation. Dev Growth Differ 2007;49:265-275. Turnpenny PD, Alman B, Cornier AS, et al: Abnormal vertebral segmentation and the notch signaling pathway in man. Dev Dyn 2007;236:1456-1474. Kappen C: Early and late functions of Hox genes in the development of the axial skeleton, in Buckwalter JA, Ehrlich MG, Sandell LJ, et al (eds): Skeletal growth and development: Clinical issues and basic science advances. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 147-162. Question #: 56 A 26-year-old man has a scaphoid waist fracture, and a decision is made for screw fixation through the dorsal approach (antegrade screw placement). Which of the following is considered the most reliable method to achieve proper screw seating below the subchondral bone? 1- Direct palpation 2- Direct visualization 3- Guide wire measurement 4- Static fluoroscopic imaging 5- Dynamic (live) fluoroscopic imaging Preferred Response: 2 Recommended Reading(s): Adamany DC, Mikola EA, Fraser BJ: Percutaneous fixation of the scaphoid through a dorsal approach: An anatomic study. J Hand Surg Am 2008;33:327-331. Tumilty JA, Squire DS: Unrecognized chondral penetration by a Herbert screw in the scaphoid. J Hand Surg Am 1996;21:66-68.
- 46. Question #: 57 While trialing a cruciate-retaining total knee arthroplasty, the knee lacks 10° of extension. When flexed beyond 90°, the tibiofemoral contact point translates posterior and there is no lift-off of the tray trial with deep flexion. What is the next most appropriate step? 1- Increase the posterior slope of the tibia 2- Resect more tibia 3- Resect more distal femur 4- Recess the posterior cruciate ligament 5- Downsize the femoral compartment Preferred Response: 3 Recommended Reading(s): Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 457-471. Question #: 58 With the development of glenohumeral internal rotation deficit in a pitcher, the humeral head is shifted in what direction during the cocking phase of throwing? 1- Anteroinferior 2- Anterosuperior 3- Posterosuperior 4- Posteroinferior 5- No change in position occurs Preferred Response: 3 Recommended Reading(s): Grossman MG, Tibone JE, McGarry MH, et al: A cadaveric model of the throwing shoulder: A possible etiology of superior labrum anterior-to-posterior lesions. J Bone Joint Surg Am 2005;87:824-831. Lintner D, Mayol M, Uzodinma O, et al: Glenohumeral internal rotation deficits in professional pitchers enrolled in an internal rotation stretching program. Am J Sports Med 2007;35:617-621.
- 47. Question #: 59 Paget’s disease of bone is associated with abnormal function of which of the following cell types? 1- Osteoblasts 2- Osteoclasts 3- Osteocytes 4- Histiocytes 5- Megakarocytes Preferred Response: 2 Recommended Reading(s): Klein GR, Parvizi J: Surgical manifestations of Paget’s disease. J Am Acad Orthop Surg 2006;14:577-586. Robey PG, Bianco P: The role of osteogenic cells in the pathophysiology of Paget’s disease. J Bone Miner Res 1999;14:9-16.
- 48. Figure 60a Figure 60b Figure 60c
- 49. Question #: 60 A 55-year-old electrician who is 5’ 10” tall and weighs 250 lbs developed severe medial compartment degenerative arthritis 6 months ago and underwent a medial unicondylar knee arthroplasty. He did extremely well initially and returned to work after 5 weeks. He reports new onset pain made worse by prolonged weight bearing and stair climbing. He has no fevers, chills, or pain at rest. Radiographs are shown in Figures 60a and 60b. A delayed image from a bone scan is shown in Figure 60c. What is most likely diagnosis? 1- Infection 2- Anterior cruciate ligament disruption 3- Osteolysis 4- Stress fracture 5- Dislodgement of polyethylene Preferred Response: 4 Recommended Reading(s): Brumby SA, Carrington R, Zayontz S, et al: Tibial plateau stress fracture: A complication of unicompartmental knee arthroplasty using 4 guide pinholes. J Arthroplasty 2003;18:809- 812. Pandit H, Murray DW, Dodd CA, et al: Medial tibial plateau fracture and the Oxford unicompartmental knee. Orthopedics 2007;30:28-31. Hamilton WG, Collier MB, Tarabee E, et al: Incidence and reasons for reoperation after minimally invasive unicompartmental knee arthroplasty. J Arthroplasty 2006;21:98-107.
- 50. Figure 61a Figure 61b Figure 61c
- 51. Question #: 61 A 46-year-old female runner without foot deformity received a steroid injection into the second metatarsophalangeal (MTP) joint for forefoot pain 3 weeks prior to running a marathon. During the race, pain was noted beneath the second MTP joint. A clinical photograph and radiographs of her foot following the race are shown in Figures 61a through 61c. What is the most likely diagnosis? 1- Plantar fascia rupture 2- Second metatarsal stress fracture 3- Hammertoe deformity 4- Plantar plate rupture with subluxation of the second MTP joint 5- Rheumatoid arthritis Preferred Response: 4 Recommended Reading(s): McGarvey WC: Second metatarsophalangeal instability, in Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction of the Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 69-75. Mizel MS, Yodlowski ML: Disorders of the lesser metatarsophalangeal joints. J Am Acad Orthop Surg 1995;3:166-173. Question #: 62 The parents of a 5-year-old boy report that he had a right clubfoot corrected using the Ponseti method shortly after birth. They now note that he has been walking on the outside of his foot. Examination reveals the forefoot and hindfoot are well corrected. The ankle can be dorsiflexed 15°. When he walks, the foot supinates during swing phase and comes down on the lateral border during stance phase. What is the preferred management of this patient? 1- Reverse last shoes 2- Split posterior tibial tendon transfer 3- Full-time use of the Denis-Browne bar for 3 months 4- Anterior tibial tendon transfer to the lateral cuneiform 5- Percutaneous heel cord tenotomy and plantar fasciotomy Preferred Response: 4 Recommended Reading(s): Ponseti IV: Relapses, in Congenital Clubfoot: Fundamentals of Treatment. New York, NY, Oxford University Press, 1996, pp 98-106. Morcuende JA, Weinstein SL, Dietz FR, et al: Plaster cast treatment of clubfoot: The Ponseti method of manipulation and casting. J Pediatr Orthop Part B 1994;3:161-167.
- 52. Question #: 63 The mechanism of action of bisphosphonates is largely dependent on 1- metabolites. 2- chemical structure. 3- route of administration. 4- synthetic characteristics. 5- bone binding properties. Preferred Response: 2 Recommended Reading(s): Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 315-330. Morris CD, Einhorn TA: Bisphosphonates in orthopaedic surgery. J Bone Joint Surg Am 2005;87:1609-1618. Question #: 64 What is the primary biomechanical role of the rotator cuff? 1- It provides the major force to move the arm forward. 2- It provides the majority of humeral rotation power. 3- It initiates arm elevation before the trapezius, serratus anterior, and deltoid are activated. 4- It compresses the humeral head against the glenoid. 5- It is the major dynamic stabilizer in the extremes of motion. Preferred Response: 4 Recommended Reading(s): Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 79-88. Hirashima M, Kadota H, Sakurai S, et al: Sequential muscle activity and its functional role in the upper extremity and trunk during overarm throwing. J Sports Sci 2002;20:301-310.
- 53. Question #: 65 Two-flap Z-plasty with 60° limbs provides how much lengthening of scar contracture? 1- 10% 2- 25% 3- 50% 4- 75% 5- 100% Preferred Response: 4 Recommended Reading(s): Hove CR, Williams EF III, Rodgers BJ: Z-plasty: A concise review. Facial Plast Surg 2001;17:289-294. Browne EZ, Pederson WC: Skin grafts and skin flaps, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, pp 1651-1692.
- 54. Figure 66a Figure 66b Figure 66c Figure 66d
- 55. Question #: 66 Figures 66a through 66d show the radiographs and MRI scans of a 68-year-old woman who reports a 1-year history of worsening low back and left leg pain. Currently she is unable to walk more than two blocks without resting. She is able to complete her grocery shopping by leaning on the cart while in the store. She has a normal neurologic exam and no significant medical comorbidities. She has failed to respond to epidural steroids and physical therapy. Which of the following treatment options offers the most likely chance to relieve her pain symptoms? 1- Anterior diskectomy and interbody fusion at L4/5 2- Left-sided laminotomy and diskectomy at L4/5 3- Complete laminectomy at L4 with partial facetectomies and foraminotomies at L4/5 4- A series of three transforaminal epidural steroid injections at L4/5 5- Laminectomy, partial facetectomy, and foraminotomy at L4/5 with posterior spinal fusion Preferred Response: 5 Recommended Reading(s): Weinstein JN, Lurie JD, Tosteson TD, et al: Surgical versus nonsurgical treatment for lumbar degenerative spondylolisthesis. N Engl J Med 2007;356:2257-2270. Knaub MA, Won DS, McGuire R, et al: Lumbar spinal stenosis: Indications for arthrodesis and spinal instrumentation. Instr Course Lect 2005;54:313-319. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-808.
- 56. Question #: 67 A 7-year-old girl has a mass on the volar radial aspect of her wrist. The mass is 1 cm in diameter, firm, and not fixed to the skin. A decision is made for excision. Before doing this, what two clinical tests should be done? 1- Adams test and Steinberg sign 2- Stagnara and Froment tests 3- Transillumination and Allen test 4- Diadochokinesia and Phalen tests 5- Digital capillary refill and blood pressure Preferred Response: 3 Recommended Reading(s): Herring JA: Kyphosis, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 413-441. Wang AA, Hutchinson DT: Longitudinal observation of pediatric hand and wrist ganglia. J Hand Surg Am 2001;26:599-602. Question #: 68 Osteogenesis imperfecta results from a mutation in which of the following genes? 1- Type I collagen 2- Type II collagen 3- Type IV collagen 4- Type VI collagen 5- Type X collagen Preferred Response: 1 Recommended Reading(s): Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 25-47. Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 773-783.
- 57. Figure 69a Figure 69b Question #: 69 A 56-year-old man has a thigh mass. He has no significant history of trauma or subcutaneous ecchymosis and is not taking anticoagulation medication. The MRI scans shown in Figures 69a and 69b confirm that this is a deep blood-filled cyst-like structure with enhancement of the cyst wall. Aspiration is consistent with old hematoma but it recurs after aspiration. What is the next most appropriate treatment option? 1- Ice, compression, and elevation 2- Open biopsy 3- Percutaneous drain placement, multiple if necessary 4- Irrigation, debridement, and placement of several drains 5- Resection of the entire mass including the cyst wall Preferred Response: 2 Recommended Reading(s): Ward WG Sr, Rougraff B, Quinn R, et al: Tumors masquerading as hematomas. Clin Orthop Relat Res 2007;465:232-240. Schwartz HS (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 59-72.
- 58. Question #: 70 Following open reduction and internal fixation of an ankle fracture, what is the time frame for patients to return to normal automobile breaking time? 1- 3 weeks 2- 6 weeks 3- 9 weeks 4- 12 weeks 5- 24 weeks Preferred Response: 3 Recommended Reading(s): Egol KA, Sheikhazadeh A, Mogatederi S, et al: Lower-extremity function for driving an automobile after operative treatment of ankle fracture. J Bone Joint Surg Am 2003;85:1185-1189. Egol KA, Sheikhazadeh A, Koval KJ: Braking function after complex lower extremity trauma. J Trauma 2008;65:1435-1438.
- 59. Figure 71a Figure 71b Figure 71c
- 60. Question #: 71 A 20-year-old man has had progressive right buttock pain. AP pelvis and lateral hip radiographs, and an MRI scan are shown in Figures 71a through 71c. He reports that he has had several “bone spurs” removed in the past in his wrist and ankles. Genotype analysis demonstrates EXT 1 expression, which implies 1- no clinical significance. 2- less severe involvement than EXT 2. 3- less likelihood of subsequent familial transmission. 4- a high likelihood of local recurrence after removal. 5- a higher risk for sarcoma development than EXT 2. Preferred Response: 5 Recommended Reading(s): Porter DE, Lonie L, Fraser M, et al: Severity of disease and risk of malignant change in hereditary multiple exostoses: A genotype-phenotype study. J Bone Joint Surg Br 2004;86:1041-1046. Alvarez C, Tredwell S, De Vera M, et al: The genotype-phenotype correlation of hereditary multiple exostoses. Clin Genet 2006;70:122-130. Question #: 72 A baseball pitcher reports posterolateral shoulder pain and lateral shoulder paresthesias when in the cocking position of throwing. What is the most likely diagnosis? 1- SLAP lesion 2- Anterior instability 3- Internal impingement 4- Posterior capsule tightness 5- Quadrilateral space syndrome Preferred Response: 5 Recommended Reading(s): Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 273-285. DeLee JC, Drez D Jr, Miller MD (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2002, p 1247.
- 61. Figure 73 Question #: 73 A 35-year-old man is seen in the emergency department with the injury shown in Figure 73. Reduction of this fracture should be performed urgently to prevent which of the following complications? 1- Subtalar arthrosis 2- Necrosis of the posterior skin 3- Malunion 4- Nonunion 5- Achilles tendon contracture Preferred Response: 2 Recommended Reading(s): Fitzgibbons TC, McMullen ST: Fractures and dislocations of the calcaneus in Heckman J, Bucholz RW (eds): Rockwood and Green’s Fractures in Adults, ed 5. New York, NY, Lippincott Williams & Wilkins, 2001, pp 2133-2174. Sanders R: Fractures and fracture-dislocations of the calcaneus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1422-1464.
- 62. Question #: 74 McCune-Albright syndrome (polyostotic fibrous dysplasia, café-au-lait spots, precocious puberty) is caused by a mutation in which of the following genes? 1- MAP kinase 2- Gs G-protein 3- Adenylyl cyclase 4- c-fos proto-oncogene 5- Parathyroid hormone receptor Preferred Response: 2 Recommended Reading(s): Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 25-47. Weinstein LS: G(s)alpha mutations in fibrous dysplasia and McCune-Albright syndrome. J Bone Miner Res 2006;21:P120-P124. Question #: 75 The Emergency Medical Treatment and Active Labor Act (EMTALA) requires that patients admitted to an emergency room cannot be transferred unless evaluated by a responsible health care provider and 1- they are screened for appropriate insurance coverage. 2- blood transfusions and other medication infusions are completed. 3- all emergent surgery is performed. 4- the benefits of transfer outweigh the risks. 5- transportation (air or ground) is less than 60 minutes. Preferred Response: 4 Recommended Reading(s): Fishgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 3-12. Koval KJ, Tingey CW, Spratt KF: Are patients being transfered to level-1 trauma centers for reasons other than medical necessity? J Bone Joint Surg Am 2006;88:2124-2132.
- 63. Question #: 76 Which of the following structures blocks successful closed reduction of a lateral subtalar dislocation? 1- Spring ligament 2- Deltoid ligament 3- Extensor digitorum brevis 4- Posterior tibial tendon 5- Extensor hallucis longus tendon Preferred Response: 4 Recommended Reading(s): Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 493-509. Bibbo C, Anderson RB, Davis WH: Injury characteristics and the clinical outcome of subtalar dislocations: A clinical and radiographic analysis of 25 cases. Foot Ankle Int 2003;24:158-163.
- 64. Figure 77a Figure 77b Question #: 77 A 12-year-old boy sustains an injury to his knee while playing football. He has immediate swelling and is unable to walk on the limb. Examination reveals he is unable to do a straight leg raise and has marked swelling anteriorly. A lateral radiograph and MRI scan are seen in Figures 77a and 77b. What is the most appropriate treatment? 1- Reconstruction of the patellar tendon 2- Surgical reduction and internal fixation 3- Immobilization in a straight cast for 6 weeks 4- Open biopsy of the mass 5- Application of a range-of-motion brace limiting flexion to 45° for 6 weeks Preferred Response: 2 Recommended Reading(s): Zionts LE: Fractures around the knee in children. J Am Acad Orthop Surg 2002;10:345- 355. Sponseller PD, Stanitski CL: Fractures and dislocations about the knee, in Beaty JH, Kasser JR (eds): Rockwood and Wilkins’ Fractures in Children, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 1029-1033.
- 65. Question #: 78 Most studies of cemented Charnley all-polyethylene acetabular shells showed a less than 5% failure rate at 10 years. What is the failure rate (revision rate) of these cups at 20 years? 1- Less than 10% 2- 15% to 20% 3- 30% to 40% 4- 60% to 70% 5- Greater than 90% Preferred Response: 2 Recommended Reading(s): Della Valle CJ, Kaplan K, Jazrawi A, et al: Primary total hip arthroplasty with a flanged cemented all-polyethylene acetabular component: Evaluation at a minimum of 20 years. J Arthroplasty 2004;19:23-26. Kavanagh BF, Wallrichs S, Dewitz M, et al: Charnley low-friction arthroplasty of the hip: Twenty-year results with cement. J Arthroplasty 1994;9:229-234. Callaghan JJ, Templeton JE, Liu SS, et al: Results of Charnley total hip arthroplasty at a minimum of thirty years: A concise follow-up of a previous report. J Bone Joint Surg Am 2004;86:690-695. Question #: 79 Which of the following individuals is considered the most ideal patient for total hip arthroplasty following a femoral neck fracture? 1- Healthy 31-year-old man with a displaced vertically oriented fracture 2- 61-year-old woman with a nondisplaced stress fracture 3- 70-year-old avid golfer 4- 81-year-old man with Parkinson’s disease 5- 93-year-old woman with dementia Preferred Response: 3 Recommended Reading(s): Blomfeldt R, Tornkvist H, Ponzer S, et al: Displaced femoral neck fracture: Comparison of primary total hip replacement with secondary replacement after failed internal fixation: A 2- year follow-up of 84 patients. Acta Orthop 2006;77:638-643. Blomfeldt R, Tornkvist H, Eriksson K, et al: A randomized controlled trial comparing bipolar hemiarthroplasty with total hip replacement for displaced intracapsular fractures of the femoral neck in elderly patients. J Bone Joint Surg Br 2007;89:160-165.
- 66. Question #: 80 A 25-year-old woman has a Boutonniere deformity of the ring finger. Which of the following mechanisms is the most likely cause of this deformity? 1- Chronic mallet finger 2- Old avulsion fracture of the central slip insertion 3- Rupture of the flexor digitorum superficialis 4- Sagittal band rupture at the metacarpophalangeal joint 5- Loss of continuity of the volar plate of the proximal interphalangeal joint Preferred Response: 2 Recommended Reading(s): Tuttle HG, Olvey SP, Stern PJ: Tendon avulsion injuries of the distal phalanx. Clin Orthop Relat Res 2006;445:157-168. Lilly SI, Messer TM: Complications after treatment of flexor tendon injuries. J Am Acad Orthop Surg 2006;14:387-396. Imatami J, Hashizume H, Wake H, et al: The central slip attachment fracture. J Hand Surg Br 1997;22:107-109. Burton RI, Melchihor JA: Extensor tendons - late reconstruction, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1988-2019.
- 67. Figure 81a Figure 81b Question #: 81 A 5-year-old boy fell in the park and sustained a closed injury to the elbow. He was initially treated with closed reduction and casting. Postreduction AP and lateral radiographs are shown in Figures 81a and 81b. At the 1-week follow-up visit, the radial head is noted to be dislocated. What is the next most appropriate step in treatment? 1- Closed reduction of the radial head and closed reduction of the ulna, with pin fixation of the ulna 2- Closed reduction of the ulna with open reduction of the radiocapitellar joint and reconstruction of the annular ligament 3- Closed reduction of the ulna and closed reduction of the radial head with pin fixation of the radiocapitellar joint 4- Open reduction of the ulna and radiocapitellar joint, with reconstruction of the annular ligament 5- Application of a joint spanning external fixator on the elbow to maintain reduction Preferred Response: 1 Recommended Reading(s): Ring D, Jupiter JB, Waters PM: Monteggia fractures in children and adults. J Am Acad Orthop Surg 1998;6:215-224. Wilkins KE: Changes in the management of Monteggia fractures. J Pediatr Orthop 2002;22:548-554.
- 68. Question #: 82 What is the central concept in rehabilitating an athlete during nonsurgical care of an isolated grade II posterior cruciate ligament tear? 1- The knee should be splinted in full extension for 6 weeks. 2- Early range of motion and quadriceps strengthening should start as soon as pain permits. 3- Open chain hamstring strengthening exercises should be initiated early. 4- Functional braces have a high rate of success in patients with persistent symptoms. 5- Patients should not return to sport until hamstring strength equals the contralateral side. Preferred Response: 2 Recommended Reading(s): Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 155-168. Margheritini F, Rihn J, Musahl V, et al: Posterior cruciate ligament injuries in the athlete: An anatomical, biomechanical and clinical review. Sports Med 2002;32:393-408.
- 69. Figure 83a Figure 83b Question #: 83 Figures 83a and 83b show the MRI scans of a 52-year-old man with a history of metastatic lung adenocarcinoma. He reports weakness involving the right leg over the last week to the extent that he is no longer able to ambulate independently. His oncologist estimates that his life expectancy is between 6 months to 1 year. His pulmonary function is stable without a need for supplemental oxygen. What treatment option offers the best potential to restore and maintain the patient’s ambulatory status? 1- Directed radiation therapy alone 2- Surgical laminectomy followed by radiation therapy 3- Combined focused radiation therapy and chemotherapy 4- Receptor-directed chemotherapy based on an open biopsy 5- Circumferential neurologic decompression and surgical stabilization with postoperative radiation therapy Preferred Response: 5 Recommended Reading(s): Schmidt MH, Klimo P Jr, Vrionis FD: Metastatic spinal cord compression. J Natl Compr Canc Netw 2005;3:711-719. Klimo P Jr, Kestle JR, Schmidt MH: Clinical trials and evidence-based medicine for metastatic spine disease. Neurosurg Clin N Am 2004;15:549-564. Patchell RA, Tibbs PA, Regine WF, et al: Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: A randomized trial. Lancet 2005;366:643-648.
- 70. Question #: 84 Implantable direct current bone stimulators decrease osteoclast activity and increase osteoblast activity by which of the following mechanisms? 1- Reduces oxygen concentration and increases local tissue pH 2- Activates calmodulin 3- Activates fibroblast growth factor receptor-3 4- Activates transmembrane calcium translocation via voltage-gated channels 5- Creates nano motion and mechanical stimulation at the fracture site Preferred Response: 1 Recommended Reading(s): Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 331-348. Otter MW, McLeod KJ, Rubin CT: Effects of electromagnetic fields in experimental fracture repair. Clin Orthop Relat Res 1998;355S:S90-S104. Question #: 85 A 62-year-old man has advanced osteoarthritis of the shoulder. Examination reveals no atrophy of the infraspinatus and good external rotation strength. A CT scan shows the glenoid version to be -10°, and there is mild posterior subluxation of the humeral head. What is the most appropriate treatment? 1- Reverse total shoulder arthroplasty 2- Hemiarthroplasty 3- Arthroscopic capsular release 4- Total shoulder arthroplasty 5- Glenoid bone block Preferred Response: 4 Recommended Reading(s): Bryant D, Litchfield R, Sandow M, et al: A comparison of pain, strength, range of motion, and functional outcomes after hemiarthroplasty and total shoulder arthroplasty in patients with osteoarthritis of the shoulder: A systematic review and meta-analysis. J Bone Joint Surg Am 2005;87:1947-1956. Gartsman GM, Roddey TS, Hammerman SM: Shoulder arthroplasty with or without resurfacing of the glenoid in patients who have osteoarthritis. J Bone Joint Surg Am 2000;82:26-34.
- 71. Question #: 86 Which of the following factors correlates most with a satisfactory clinical outcome when managing an intra-articular fracture of the proximal tibia? 1- Age 2- Type of graft substitute 3- Condylar widening 4- Maintenance of mechanical axis 5- Degree of residual articular incongruency Preferred Response: 4 Recommended Reading(s): Rademakers MV, Kerkhoffs GM, Sierevelt IN, et al: Operative treatment of 109 tibial plateau fractures: Five- to 27-year follow-up results. J Orthop Trauma 2007;21:5-10. Weigel DP, Marsh JL: High-energy fractures of the tibial plateau: Knee function after longer follow-up. J Bone Joint Surg Am 2002;84:1541-1551. Stevens DG, Beharry R, McKee MD, et al: The long-term functional outcome of operatively treated tibial plateau fractures. J Orthop Trauma 2001;15:312-320. Honkonen SE: Degenerative arthritis after tibial plateau fractures. J Orthop Trauma 1995;9:273-277. Honkonen SE: Indications for surgical treatment of tibial condyle fractures. Clin Orthop Relat Res 1994;302:199-205.
- 72. Figure 87a Figure 87b Question #: 87 A 5-month-old girl with a dislocated left hip has been treated in a Pavlik harness full-time for the last 4 weeks. An ultrasound obtained with the patient in the harness is shown in Figures 87a and 87b. Based on these image findings, what is the next step in treatment? 1- Arthrogram, closed reduction, and hip spica casting 2- MRI arthrogram to further assess obstacles to reduction 3- Continued use of the Pavlik harness for 4 more weeks 4- Change to an Ilfeld splint for 3 more months of abduction splinting 5- Open reduction and innominate osteotomy Preferred Response: 1 Recommended Reading(s): Guille JT, Pizzutillo PD, MacEwen GD: Development dysplasia of the hip from birth to six months. J Am Acad Orthop Surg 2000;8:232-242. Mubarak S, Garfin S, Vance R, et al: Pitfalls in the use of the Pavlik harness for treatment of congenital dysplasia, subluxation, and dislocation of the hip. J Bone Joint Surg Am 1981;63:1239-1248. Weinstein SL, Mubarak SJ, Wenger DR: Developmental hip dysplasia and dislocation: Part II. Instr Course Lect 2004;53:531-542.
- 73. Question #: 88 Resident work hour guidelines should increase patient safety by decreasing resident fatigue. However, there is concern that safety benefits may be offset by the need for changes in systems of patient care necessitated by these guidelines. Which of these changes has caused the most concern for patient safety? 1- Night float rotations 2- Urgent surgery done the next day instead of on call 3- Home call 4- Decreased continuity of care 5- Use of physician extenders instead of residents Preferred Response: 4 Recommended Reading(s): Friedlander GE: The 80-hour duty week: Rationale, early attitudes, and future questions. Clin Orthop Relat Res 2006;449:138-142. Horwitz LI, Moin T, Krumholz HM, et al: Consequences of inadequate sign-out for patient care. Arch Intern Med 2008;168:1755-1760. Okie S: An elusive balance: Residents’ work hours and the continuity of care. N Engl J Med 2007;356:2665-2667. Question #: 89 Following total knee arthroplasty with resurfacing of the patella, a patient has lateral subluxation of the patella. What issue with the components is a cause of this complication? 1- Lateral placement of the tibial tray 2- Reduced composite thickness of the patella 3- External rotation of the femoral component 4- Internal rotation of the tibial component 5- Posterior translation of the femoral component Preferred Response: 4 Recommended Reading(s): Malo M, Vince KG: The unstable patella after total knee arthroplasty: Etiology, prevention, and management. J Am Acad Orthop Surg 2003;11:364-371.
- 74. Question #: 90 What anatomic structure inserts most anteriorly on the proximal fibula? 1- Sartorius 2- Iliotibial band 3- Biceps femoris 4- Popliteofibular ligament 5- Lateral collateral ligament Preferred Response: 5 Recommended Reading(s): LaPrade RF, Ly TV, Wentorf FA, et al: The posterolateral attachments of the knee: A qualitative and quantitative morphologic analysis of the fibular collateral ligament, popliteus tendon, popliteofibular ligament, and lateral gastrocnemius tendon. Am J Sports Med 2003;31:854-860. Stannard JP, Brown SL, Farris RC, et al: The posterolateral corner of the knee: Repair versus reconstruction. Am J Sports Med 2005;33:881-888.
- 75. Figure 91 Question #: 91 What nerve is most at risk when placing the intramedullary device shown in Figure 91? 1- Lateral plantar 2- Medial plantar 3- Deep peroneal 4- Saphenous 5- Medial calcaneal Preferred Response: 1 Recommended Reading(s): Flock TJ, Ishikawa S, Hecht PJ, et al: Heel anatomy for retrograde tibiotalocalcaneal roddings: A roentgenographic and anatomic analysis. Foot Ankle Int 1997;8:233-235. Pochatko DJ, Smith JW, Phillips RA, et al: Anatomic structures at risk: Combined subtalar and ankle arthrodesis with a retrograde intramedullary rod. Foot Ankle Int 1995;16:542- 547.
- 76. Figure 92a Figure 92b Figure 92c Figure 92d
- 77. Question #: 92 A 67-year-old woman reports knee and calf pain after mild exercise, and states that the pain is relieved by rest. She notes that radiographs were obtained 5 years ago and again recently. Figure 92a is from 5 years prior. Figure 92b is current. Current CT scans of the distal femur are seen in Figures 92c and 92d. What is the next most appropriate step in treatment? 1- Vascular surgery consultation 2- Biopsy and radiofrequency ablation 3- Biopsy, neoadjuvant chemotherapy, and resection 4- Biopsy, curettage, and filling the void with methylmethacrylate 5- Distal femoral resection and metal endoprosthetic reconstruction Preferred Response: 1 Recommended Reading(s): Skeletal Lesions Interobserver Correlation Among Expert Diagnosticians (SLICED) Study group: Reliability of histopathologic and radiologic grading of cartilaginous neoplasms in long bones. J Bone Joint Surg Am 2007;89:2113-2123. Ryzewicz M, Manaster BJ, Naar E, et al: Low-grade cartilage tumors: Diagnosis and treatment. Orthopaedics 2007;30:35-46.
- 78. Figure 93 Question #: 93 The injury shown in Figure 93 is associated with which of the following? 1- Child abuse 2- Folic acid deficiency 3- Osteogenesis imperfecta 4- Hypophosphatemic rickets 5- Generalized joint hypermobility Preferred Response: 1 Recommended Reading(s): DeLee JC, Wilkins KE, Rogers LF, et al: Fracture-separation of the distal humeral epiphysis. J Bone Joint Surg Am 1980;62:46-51. Akbarnia BA, Silberstein MJ, Rende RJ, et al: Arthrography in the diagnosis of fractures of the distal end of the humerus in infants. J Bone Joint Surg Am 1986;68:599-602.
- 79. Question #: 94 What is the most common cause of hematogenous osteomyelitis in sickle cell disease? 1- Salmonella 2- Propionibacterium 3- Enterobacteriaceae 4- Bartonella henselae 5- Pseudomonas aeruginosa Preferred Response: 1 Recommended Reading(s): Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 301-318. Cornwall R, Dormans JP: Diseases of the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, pp 357-404. Question #: 95 Patients with multiple hereditary osteochondromas frequently have loss of forearm rotation and ulnar shortening. What procedure is most likely to improve forearm rotation in these patients? 1- Tendon transfer 2- Ulnar lengthening 3- Radial head excision 4- Distal ulnar resection 5- Simple excision of the osteochondroma Preferred Response: 5 Recommended Reading(s): Shin EK, Jones NF, Lawrence JF: Treatment of multiple hereditary osteochondromas of the forearm in children: A study of surgical procedures. J Bone Joint Surg Br 2006;88:255-260. Akita S, Murase T, Yonenobu K, et al: Long-term results of surgery for forearm deformities in patients with multiple cartilaginous exostoses. J Bone Joint Surg Am 2007;89:1993- 1999.
- 80. Question #: 96 Partial distal biceps tendon tears occur primarily on which side of the tuberosity footprint? 1- Radial 2- Ulnar 3- Proximal 4- Distal 5- Central Preferred Response: 1 Recommended Reading(s): Kelly EW, Steinmann S, O’Driscoll SW: Surgical treatment of partial distal biceps tendon ruptures through a single posterior incision. J Shoulder Elbow Surg 2003;12:456-461. Davis WM, Yassine Z: An etiological factor in tear of the distal tendon of the biceps brachii: Report of two cases. J Bone Joint Surg Am 1956;39:1365-1368. Question #: 97 What is the preferred treatment for a 50% laceration of the flexor tendons with triggering? 1- Core 4/0 suture repair 2- Core 4/0 suture repair with 6/0 peritendinous suture 3- Epitendinous repair with 4/0 suture 4- Epitendinous repair with 6/0 suture 5- Trimming of frayed edges Preferred Response: 5 Recommended Reading(s): Bishop AT, Cooney WP III, Wood MB: Treatment of partial flexor tendon lacerations: The effect of tenorrhaphy and early protected mobilization. J Trauma 1986;26:301-312. McGeorge DD, Stillwell JH: Partial flexor tendon injuries: To repair or not. J Hand Surg Br 1992;17:176-177.
- 81. Figure 98a Figure 98b Figure 98c Figure 98d
- 82. Question #: 98 A 52-year-old man was involved in a motor vehicle accident and now reports severe low back pain and left anterior leg and foot paresthesias. Radiographs and CT scans are shown in Figures 98a through 98d. He has no lower extremity weakness. He is otherwise hemodynamically stable and neurologically intact. What is the most appropriate management? 1- Thoracolumbosacral orthosis and mobilization 2- Anterior vertebrectomy, vertebral body reconstruction, and plating 3- Posterior L5 laminectomy 4- Posterior L5 laminectomy and L4-S1 posterolateral fusion 5- Transpedicular reduction of intracanal fragments Preferred Response: 1 Recommended Reading(s): Butler JS, Fitzpatrick P, Ni Mhaolain AM, et al: The management and functional outcome of isolated burst fractures of the fifth lumbar vertebra. Spine 2007;32:443-447. Seybold EA, Sweeney, CA, Fredrickson BE, et al: Functional outcome of low lumbar burst fractures: A multicenter review of operative and nonoperative treatment of L3-L5. Spine 1999;24:2154-2161.
- 83. Question #: 99 Which of the following arteries connect the obturator to the external iliac? 1- Corona mortis 2- Recurrent obturator 3- Circumflex magnus 4- Hypogastric branches of the deep internal iliac 5- Ascending pudendal communicating branches Preferred Response: 1 Recommended Reading(s): Tornetta P III, Hochwald N, Levine R: Corona mortis: Incidence and location. Clin Orthop Relat Res 1996;329:97-101. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. New York, NY, Springer-Verlag, 1993, pp 375-381. Question #: 100 The most common cause of a malpractice suit against an orthopaedic surgeon involves treatment of which of the following conditions? 1- Femoral fracture 2- Humeral fractures with nerve palsy 3- Knee arthroplasty 4- Meniscal tear 5- Spinal stenosis Preferred Response: 1 Recommended Reading(s): Femur fracture care frequent cause of lawsuit. Managing Orthopaedic Malpractice Risk, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001 Bulletin. http://www2.aaos.org/aaos/archives/bulletin/feb01/fline4.htm. Accessed on July 24, 2009.
- 84. Figure 101a Figure 101b Figure 101c
- 85. Question #: 101 A 12-year-old boy has had pain in the right knee for the past 6 weeks. He has had two episodes of giving way but no locking. He denies any history of injury. Examination reveals no effusion, ligaments are stable, range of motion is full, and there is no localized tenderness. An AP radiograph and MRI scans are shown in Figures 101a through 101c. What is the most appropriate management? 1- Excision of the lesion 2- Retrograde drilling of the lesion 3- Antegrade drilling of the lesion 4- Arthroscopic reduction and fixation 5- Observation and limitation of activities Preferred Response: 5 Recommended Reading(s): Schenck RC Jr, Goodnight JM: Osteochondritis dissecans. J Bone Joint Surg Am 1996;78:439-456. Herring JA: Disorders of the knee, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 919-971. Question #: 102 What muscle groups are weakest after antegrade intramedullary nailing of a midshaft femoral fracture? 1- Hamstrings and abductors 2- Hamstrings and adductors 3- Quadriceps and abductors 4- Quadriceps and external rotators 5- Abductors and external rotators Preferred Response: 3 Recommended Reading(s): Kapp W, Lindsey RW, Noble PC, et al: Long-term residual musculoskeletal deficits after femoral shaft fractures treated with intramedullary nailing. J Trauma 2000;49:446-449. Archdeacon M, Ford KR, Wyrick J, et al: A prospective functional outcome and motion analysis evaluation of the hip abductors after femur fracture and antegrade nailing. J Orthop Trauma 2008;22:3-9.
- 86. Question #: 103 Which of the following surgical approaches to the hip uses an internervous plane? 1- Posterolateral 2- Posterior lateral (Moore) 3- Anterior (Smith-Peterson) 4- Anterolateral (Watson-Jones) 5- Direct lateral (Hardinge) Preferred Response: 3 Recommended Reading(s): Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 311-321. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 1994, pp 325-335. Question #: 104 Which of the following methods of antibiotic treatment has been associated with the highest success rate in diabetic patients treated nonsurgically for osteomyelitis of the foot? 1- Vancomycin IV antibiotic 2- Dual drug oral antibiotics 3- IV antibiotics based on a bone biopsy 4- IV antibiotics based on a swab of the open wound 5- IV antibiotics based on the hospital profile of the most common organisms Preferred Response: 3 Recommended Reading(s): Senneville E, Lombart A, Beltrand E, et al: Outcome of diabetic foot osteomyelitis treated nonsurgically: A retrospective cohort study. Diabetes Care 2008;31:637-642. Lipsky BA: Infectious problems of the foot in diabetic patients, in Bowker JH, Pfeifer MA (eds): Levin and O’Neal’s The Diabetic Foot, ed 6. St Louis, MO, Mosby, 2001, pp 467- 480.
- 87. Question #: 105 Which of the following is considered the most important portion of the kinetic chain in protecting the thrower’s elbow from valgus loads? 1- Forearm pronation 2- Scapular retraction 3- Scapular protraction 4- Glenohumeral internal rotation 5- Glenohumeral external rotation Preferred Response: 4 Recommended Reading(s): Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 101-111. Marshall RN, Elliott BC: Long-axis rotation: The missing link in proximal-to-distal sequencing. J Sports Sci 2000;18:247-254.
- 88. Figure 106 Question #: 106 Figure 106 shows the MRI arthrogram of an 18-year-old football player who injured his shoulder. What physical examination finding is most likely to demonstrate his pathology? 1- Jerk test 2- Gerber lift-off test 3- O’Brien test 4- Sulcus sign 5- Apprehension sign Preferred Response: 1 Recommended Reading(s): Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 53-77. Millett PJ, Clavert P, Hatch GF III, et al: Recurrent posterior shoulder instability. J Am Acad Orthop Surg 2006;14:464-467.
- 89. Question #: 107 Which of the following findings on microscopy best characterizes the pathologic features of lateral epicondylitis? 1- Giant cell infiltration 2- Cystic degeneration with Rice bodies and fatty infiltration 3- Localized hemorrhage with proliferation of neutrophils 4- Fibroblast hypertrophy, disorganized collagen, and vascular hyperplasia 5- Hypertrophic collagen fibers, mature fibroblasts, and frequent macrophages Preferred Response: 4 Recommended Reading(s): Kraushaar BS, Nirschl RP: Tendinosis of the elbow (tennis elbow): Clinical features and findings of histological, immunohistochemical, and electron microscopy studies. J Bone Joint Surg Am 1999;81:259-278. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 271-284. Nirschl RP, Pettrone FA: Tennis elbow: The surgical treatment of lateral epicondylitis. J Bone Joint Surg Am 1979;61:832-839. Question #: 108 What method of terminal polyethylene sterilization results in the greatest number of remaining free radicals within the polyethylene? 1- Gas plasma 2- Ethylene oxide 3- Gamma irradiation 4- Gamma irradiation and annealing 5- Gamma irradiation and remelting Preferred Response: 3 Recommended Reading(s): Gordon AC, D’Lima DD, Colwell CW Jr: Highly cross-linked polyethylene in total hip arthroplasty. J Am Acad Orthop Surg 2006;14:511-523. McKellop H, Shen FW, Lu B, et al: Effect of sterilization method and other modifications on the wear resistance of acetabular cups made of ultra-high molecular weight polyethylene: A hip-simulator study. J Bone Joint Surg Am 2000;82:1708-1725.
- 90. Question #: 109 Which of the following conditions has little or no published data to support the use of locked plating techniques? 1- Proximal intra-articular bicondylar tibia fracture 2- Proximal humeral fracture 3- Bicondylar distal femur fracture 4- A geriatric periprosthetic fracture 5- Hypertrophic humeral nonunion in a young male Preferred Response: 5 Recommended Reading(s): Haidukewych GJ, Ricci W: Locked plating in orthopaedic trauma: A clinical update. J Am Acad Orthop Surg 2008;16:347-355. Question #: 110 The halo vest is least effective at controlling which of the following spinal motions? 1- Lateral bend 2- Flexion 3- Extension 4- Axial rotation 5- Axial distraction Preferred Response: 5 Recommended Reading(s): Ivancic PC, Beauchman NN, Tweardy: Effect of halo-vest components on stabilizing the injured cervical spine. Spine 2009;34:167-175. Johnson RM, Hart DL, Simmons EF, et al: Cervical orthoses: A study comparing their effectiveness in restricting cervical motion in normal subjects. J Bone Joint Surg Am 1977;59:332-339.
- 91. Figure 111a Figure 111b Figure 111c
- 92. Question #: 111 An 11-year-old girl has had neck pain for the past 6 months. She has had no neurologic symptoms and is neurologically normal on physical examination. Cervical spine range of motion is normal. An open-mouth view and flexion and extension radiographs are seen in Figures 111a through 111c. What is the most appropriate treatment? 1- Cessation of contact sports 2- Decompressive laminectomy 3- Anterior cervical spinal fusion 4- Posterior cervical spinal fusion 5- Anterior and posterior cervical spinal fusion Preferred Response: 4 Recommended Reading(s): Reilly CW, Choit RL: Transarticular screws in the management of C1-C2 instability in children. J Pediatr Orthop 2006;26:582-588. Sankar WN, Wills BP, Dormans JP, et al: Os odontoideum revisited: The case for a multifactorial etiology. Spine 2006;31:979-984. Question #: 112 A review of a patient’s AP pelvis and oblique (Judet) radiographs reveals that the iliopectineal line is intact, the ilioischial line is disrupted, and there is a fracture of the inferior pubic ramus. Based on these findings, what is the most likely acetabular fracture pattern? 1- Transverse 2- Transverse and posterior wall 3- Posterior wall 4- Posterior column 5- T-type Preferred Response: 4 Recommended Reading(s): Letournel E: Acetabulum fractures: Classification and management. Clin Orthop Relat Res 1980;151:81-106. Patel V, Day A, Dinah F, et al: The value of specific radiological features in the classification of acetabular fractures. J Bone Joint Surg Br 2007;89:72-76.
- 93. Question #: 113 The most effective method for nonsurgical management of a chronic (symptoms lasting greater than 3 months) flexible acquired adult flatfoot deformity is with which of the following devices? 1- UCBL orthosis 2- Ankle-foot orthosis 3- Patellar tendon-bearing orthosis 4- Indepth shoe with total contact foot orthosis 5- Indepth shoe with extended medial counter and medial flare Preferred Response: 2 Recommended Reading(s): Alvarez, RG, Marini A, Schmitt C, et al: Stage I and II posterior tibial tendon dysfunction treated by a structured nonoperative management protocol: An orthosis and exercise program. Foot Ankle Int 2006;27:2-8. Augustin JF, Lin SS, Berberian WS, et al: Nonoperative treatment of the adult acquired flat foot with the Arizona brace. Foot Ankle Clin 2003;8:491-502. Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741. Question #: 114 When performing a lateral column lengthening procedure with a posterior tibial tendon reconstruction for correction of an acquired adult flatfoot deformity, what procedure is also commonly required? 1- Talar neck osteotomy 2- Lengthening of the gastrocsoleus complex 3- First metatarsophalangeal joint fusion 4- Lateral ankle ligament reconstruction 5- Peroneus longus to brevis tendon transfer Preferred Response: 2 Recommended Reading(s): Myerson MS: Adult acquired flatfoot deformity: Treatment of dysfunction of the posterior tibial tendon. Instr Course Lect 1997;46:393-405. Pinney SJ, Lin SS: Current concepts review: Acquired adult flatfoot deformity. Foot Ankle Int 2006;27:66-75.
- 94. Question #: 115 The amount of energy per volume that a material can absorb prior to failure defines which of the following terms? 1- Toughness 2- Failure point 3- Viscoelasticity 4- Fatigue strength 5- Young’s modulus Preferred Response: 1 Recommended Reading(s): Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 49-64. Chao EYS, Aro HT: Biomechanics of fracture fixation, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics. New York, NY, Raven Press, 1991, pp 293-336. Question #: 116 Which of the following postoperative modalities to prevent deep venous thrombosis is associated with the highest risk of hematoma? 1- Aspirin 2- Dipyridamole 3- Compression device 4- Clopidogrel bisulfate 5- Low-molecular-weight heparin Preferred Response: 5 Recommended Reading(s): Dorr LD, Gendelman V, Maheshwari AV, et al: Multimodal thromboprophylaxis for total hip and knee arthroplasty based on risk assessment. J Bone Joint Surg Am 2007;89:2648- 2657. Lee MC, Nickisch F, Limbird RS: Massive retroperitoneal hematoma during enoxaperan treatment of pulmonary embolism after primary total hip arthroplasty: Case-reports and review of the literature. J Arthoroplasty 2006;21:1209-1214.
- 95. Figure 117a Figure 117b Figure 117c Question #: 117 A 4-year-old girl has bowleg deformities. Radiographs of her lower and upper extremities are shown in Figures 117a through 117c. She is below the 25th percentile for height. Which of the following laboratory findings are most likely to be present? 1- Normal serum Ca; low serum phosphate; elevated alkaline phosphatase 2- Low serum Ca; normal serum phosphate; elevated alkaline phosphatase 3- Low serum Ca; elevated serum phosphate; low alkaline phosphatase 4- Elevated serum Ca; low serum phosphate; low alkaline phosphatase 5- Elevated serum Ca; elevated serum phosphate; elevated alkaline phosphatase Preferred Response: 1 Recommended Reading(s): Loeffler RD Jr, Sherman FC: The effect of treatment on growth and deformity in hypophosphatemic vitamin D-resistant rickets. Clin Orthop Relat Res 1982;162:4-10. Ferris B, Walker C, Jackson A, et al: The orthopaedic management of hypophosphatemic rickets. J Pediatr Orthop 1991;11:367-373.
- 96. Figure 118a Figure 118b Question #: 118 What plating strategy provides the most optimal fixation for the fracture seen in Figures 118a and 118b? 1- Lateral locking plate 2- Posteromedial plate 3- Lateral buttress plate 4- Anteromedial plate 5- Medial and lateral plates Preferred Response: 2 Recommended Reading(s): Georgiadis GM: Combined anterior and posterior approaches for complex tibial plateau fractures. J Bone Joint Surg Br 1994;76:285-289. Bhattacharyya T, McCarty LP III, Harris MB, et al: The posterior shearing tibial plateau fracture: Treatment and results via a posterior approach. J Orthop Trauma 2005;19:305- 310.
- 97. Question #: 119 In lateral epicondylitis, the area of tendinopathy is classically located at the origin of the 1- anconeus. 2- extensor digitorum. 3- extensor carpi ulnaris. 4- extensor carpi radialis longus. 5- extensor carpi radialis brevis. Preferred Response: 5 Recommended Reading(s): Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 91-99. Nirschl RP, Pettrone FA: Tennis elbow: The surgical treatment of lateral epicondylitis. J Bone Joint Surg Am 1979;61:832-839. Question #: 120 Warfarin is commonly used to prevent deep venous thrombosis after total hip arthroplasty. What is its mechanism of action? 1- Forms complexes with antithrombin III 2- Inactivates active thrombin and active factor Xa 3- Prevents conversion of fibrinogen to fibrin 4- Prevents gamma carboxylation in factor X and prothrombin 5- Prevents thromboxane A2 formation, interfering with platelet aggregation Preferred Response: 4 Recommended Reading(s): Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 395-413. Lieberman JR, Hsu WK: Prevention of venous thromboembolic disease after total hip and knee arthroplasty. J Bone Joint Surg Am 2005;87:2097-2112.
- 98. Figure 121a Figure 121b Question #: 121 Figures 121a and 121b show the radiographs of an otherwise healthy 42-year-old man who sustained a left ankle injury in a fall on stairs. The ankle is maintained in a position of external rotation and proves irreducible with closed efforts under general anesthesia. What anatomic structure is serving as a hindrance to reduction? 1- Peroneus longus 2- Tibialis posterior 3- Tibialis anterior 4- Ruptured deltoid ligament 5- Posterolateral tibial ridge Preferred Response: 5 Recommended Reading(s): Beekman R, Watson JT: Bosworth fracture-dislocation and resultant compartment syndrome. J Bone Joint Surg Am 2003;85:2211-2214. Hoblitzell RM, Ebraheim NA, Merritt T, et al: Bosworth fracture-dislocation of the ankle: A case report and review of the literature. Clin Orthop Relat Res 1990;255:257-262. Mayer PJ, Evarts CM: Fracture-dislocation of the ankle with posterior entrapment of the fibula behind the tibia. J Bone Joint Surg Am 1978;60:320-324. Perry CR, Rice S, Rao A, et al: Posterior fracture-dislocation of the distal part of the fibula: Mechanism and staging of injury. J Bone Joint Surg Am 1983;65:1149-1157. Szalay MD, Roberts JB: Compartment syndrome after Bosworth fracture-dislocation of the ankle: A case report. J Orthop Trauma 2001;15:301-303. White SP, Pallister I: Fracture-dislocation of the ankle with fixed displacement of the fibula behind the tibia-a rare variant. Injury 2002;33:292-294.