
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Obstetric fistulae
Ähnlich wie Obstetric fistulae (20)
Mehr von SREEVIDYA UMMADISETTI
Mehr von SREEVIDYA UMMADISETTI (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Obstetric fistulae
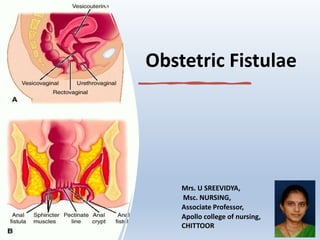
- 1. Obstetric Fistulae Mrs. U SREEVIDYA, Msc. NURSING, Associate Professor, Apollo college of nursing, CHITTOOR
- 2. PRE-TEST 1. Obstetrical fistula is best defined as: A) A hole between the vagina and the bladder or rectum B) An hole in perineum C) A hole in the uterus D) An injury to the cervix
- 3. 2. Which of the following is NOT a risk factor of developing an obstetrical fistula A) Being a young first time mother B) Being over age 35 at the time of delivery (advanced maternal age) C) Having (untrained) family members as birth attendants D) Poor nutritional status
- 4. 3. What is a rectovaginal fistula? A) A hole connecting the bladder to the vagina B) A hole connecting the vagina to the uterus C) A hole connecting the rectum to the vagina D) Any hole on the rear wall of the vagina
- 5. 4. Most common cause of VVF in india is: A) Obstructed labour B) Gynaec surgery C) Radiation D) Trauma
- 6. 5. Postpartum VVF is best repaired after: A. 6 weeks B. 8 weeks C. 3 months D. 6 months
- 7. 6. Mrs A, 48yrs had hysterectomy. On seventh day, she devoloped fever, burning micturition & continous dribbling of urine. She can also pass urine voluntarily. The diagnosis is, A. V V F B. Ureterovaginal fistula C. Stress incontinence D. Urge incontinence
- 8. 7.Most useful preoperative investigation for VVF is: A. Three swab test B. Cystoscopy C. Ultrasound D. Urine culture
- 9. 8. If RVF is present in high up(upper part ) preliminary treatment should be: A. Colostomy B. Colporraphy C. Primary repair D. Anterior resection
- 10. OBSTETRICAL FISTULA • Obstetrical fistula is a life changing childbirth injury. • An obstetrical fistula is a hole or connection that occurs between the vagina and the bladder or between the vagina and rectum. This is most often caused during a prolonged labor when the fetus' head applies continuous pressure to the pelvic bones resulting in soft tissue damage to the muscles in the pelvis.
- 11. Definition – obstetric fistula is an abnormal communication between the vagina and the bladder or rectum. – Occurred in the course of pregnancy and results in uncontrolled passage of urine, feaces or flatus into the vagina.
- 17. Causes • Obstetrical • Gynaecological 1.Obstetrical causes – Ishemic: Due to prolonged compression effect on the bladder base between the head and pubic symphysis eg : obstructed labour Traumatic : • Instrumental vaginal delivery – in destructive operation, forceps delivery • Abdominal operation – Hysterectomy for rupture uterus, LSCS
- 18. 2. Gynaecological causes • Operative Injury – Ant. Colporraphy, Abdominal hysterectomy • Traumatic - ant. Vaginal wall & bladder may be injured following fall on a pointed objects, by a stick used for criminal abortion • Malignancy – by direct spread in cases of Advanced carcinoma of cervix, vagina or bladder • Radiation - Due to radiation effect ishemic necrosis may occur
- 19. Types • Simple - Healthy tissues with good access • Complicated – Tissue loss, scarring, difficult access associated with RVF Depending upon SITE of the Fistula – Juxtacervical :( close to cx) –communication between supratrigonal region of bladder and vagina Midvaginal : communication between base (Trigone) of bladder and vagina Juxtaurethral: communication between neck of bladder and vagina
- 23. Common Symptoms The complete urinary incontinence that is describing as a common symptom, as is bowel incontinence. However, women will often report several different symptoms. Common symptoms include the following: • Constant urine leaking from vagina • Irritation of the external genitalia • Frequent urinary tract infections • Leakage of gas and/or feces into the vagina if associated with RVF • Vaginal discharge (Foul discharges) • Nausea/vomiting • Abdominal or pelvic pain • Amenorrhea (or the absence of a normal menstrual period) • Dyspareunia (painful sex) • Psychosocial problems- social refuse; depression, low self-esteem, and insomnia
- 30. Management • Prophylaxis • Immediate management– once the diagnosis is made ,continuous catherization for 6-8 days is maintained. • Operative – surgery is the choice for definitive management
- 32. Management cont.. Immediate management • If there is access to treatment immediately following birth injury, a catheter to be placed into the bladder which allows it to remain empty. • This takes pressure off of the hole, and prevents liquid from flowing through it while it repairs itself. • Doing this often allows it to heal on its own.
- 33. Non-invasive treatment options There are some non-invasive treatment options available. These have less risk than traditional surgery, including less risk of infection and a faster healing time. But they work best for small holes. Two options are avaliable, either fibrin glue, which is medical grade glue that can be used to seal the connection. Or, could use a plug, which is a matrix made from collagen used to seal the connection. • Psychosocial counseling and rehabilitation
- 34. Definitive Surgery • Ideal time for surgery is after 3 months following delivery • Surgical Fistula– If recognised <24 hrs: immediate repair If recognised >24 hrs : repair after 3 months • Radiation Fistula : repair after 12 months
- 35. Surgical Management • FISTULA REPAIR IS NOT AN EMERGENCY • Most surgeons advise waiting at least 3 months from time of injury before operating. • In the early months, the surrounding tissues are oedematous and hyperemic, making them friable and difficult to handle.
- 37. Preoperative care • Improve the patient’s general condition- Nutrition, Infection, Dermatitis, Urine acidification, Psyche. • Contractures should be treated before surgery if possible. • Encourage liberal clear fluid intake until about 4hrs before surgery. • Bowel preparation should include enema the night before.
- 38. Intraoperative Care • Anesthesia: Spinal or GA • Antibiotics: broad spectrum • Suture material: – Vicryl 2-0 - bladder and vagina – Polydioxanone 4-0 - ureter
- 40. ROUTE OF REPAIR • Depends upon access to the fistula site, mobility of the vagina and surgeon expertise. SITE APPROACH LOW FISTULA Urethral Juxtaurethral VAGINAL CIRCUMFERENTIAL LOSS OF BLADDER NECK COMBINED ABDOMINOVAGINAL MIDVAGINAL FISTULA TRANSVAGINAL HIGH VAGINAL FISTULA Post hysterectomy Juxtacervical ABDOMINAL OR VAGINAL
- 41. Principles of fistula repair • First attempt is best . Tissue mobilization Hemostasis Adequate exposure Aseptic measures Tension free closure Reinforcement Expertise
- 42. Repair of Vesicovaginal Fistula • Vaginal approach – Flap splitting technique – Saucerization – Latzko technique • Abdominal approach – Transvesical repair – Transperitoneal repair – Combined repair
- 47. Abdominal approach • Indications – High inaccessible fistula – Multiple fistulas – Involvement of uterus or bowel – Need for ureteral re-implantation – Complex fistula
- 49. Post-operative care cont.. • Maintain output at 100ml / hr • Antimicrobials • Plenty of fluids for continuous bladder drainage • Watch for any bladder block, fluid imbalance
- 50. Discharge Advice • Topass urine frequently • Avoid sexual intercourse for at least 3 months • Todefer pregnancy for at least 1 year • Subsequent deliveries should be abdominal • If repair fails, local repair should be reattempted after 3 months
- 52. Definition Abnormal communication between the rectum and vagina with involuntry escape of flatus and or feces into vagina is called RVF.
- 54. Causes 1-Acquired 2- Congenital Acquired – Obstetrical causes – • Incomplete healing or unrepaired recent complete perineal tear is commonest. • Obstructed labour- During obstructed labour the compression effect produces necrosis →infection→ sloughing→ fistule
- 55. • Instrumental injury inflicted during destructive operation Gynaecological – • Following incomplete healing of repaired surgeries • Trauma during operative procedure • Malignancy of vagina, cervix or bowel • Radiation • Fall on sharp object
- 56. Congenital – Anal canal may open into vestibule or in vagina congenitally.
- 57. • Clinical presentation: • Involuntary escape of flatus and/or feces into the vagina • Foul smelling vaginal discharge with periodic uncontrolled escape of gas • Appear immediately or 7-10 days after delivery
- 58. Diagnosis • History collection • Rectovaginal examination – size & shape of fistula. • Confirmation done by probe passing through vagina into rectum.
- 59. • Confirmation –Thin Probe is passed from the vagina through the fistulous tract into the rectum/anal canal – Methylene blue dye test – Examination under anaesthesia INVESTIGATIONS – Barium enema – Gastrograffin Enema – Barium meal to confirm intestinal fistula – Sigmoidoscopy & proctoscopy – CT scans – MRI – Ultrasound
- 60. CLASSIFICATION • Based on anatomical location of vaginal opening – Low - vaginal opening near the posterior fourchette – Mid - from the level of the cervix to just superior to the posterior fourchette – High -the fistula is in the area of the posterior fornix. • Simple vs Complex – Simple are small fistulas – Complex are large
- 61. Treatment • Preventive • Good intranatal care • Identification of simple abnormalities & repair it • Care during gynaecological surgeries • Surgery • Situated in low down- simple repair • Situated in middle third – repair by flap method • Situated high up- Preliminary colostomy→local repair after 3 wks→closure of colostomy after 3 wks
- 62. • SURGERY Route: – Transvaginal Approach – Transanal Approach – Abdominal Approach Timing: – Wait 8-12 weeks before surgical intervention to allow surrounding inflammation to resolve completely
- 63. Lifestyle and home remedies Good hygiene can help ease discomfort and reduce the chance of vaginal or urinary tract infections while waiting for repair. Other home remedies for people living with a rectovaginal fistula include: •Wash with water. Shower or gently wash outer genital area with just warm water each time when experience vaginal discharge or passage of stool. •Avoid irritants. Soap can dry and irritate the skin, but it may need a gentle unscented soap in moderation. Avoid harsh or scented soap and scented tampons and pads. Vaginal douches can increase the chance of infection. •Dry thoroughly. Allow the area to air-dry after washing, or gently pat the area dry with a clean cloth or towel.
- 64. •Avoid rubbing with dry toilet paper. Pre-moistened, alcohol- free, unscented towelettes or wipes or moistened cotton balls are a good alternative. •Apply a cream or powder. Moisture-barrier creams protect irritated skin from liquid or stool. Nonmedicated talcum powder or cornstarch also may help relieve discomfort. Be sure the area is clean and dry before you apply any cream or powder. •Wear cotton underwear and loose clothing. Tight clothing can restrict airflow and worsen skin problems. Change soiled underwear quickly. Products such as absorbent pads, disposable underwear or adult diapers can help when passing liquid or stool, but be sure they have an absorbent layer on top.
- 65. POST-TEST 1. Obstetrical fistula is best defined as: A) A hole between the vagina and the bladder or rectum B) An hole in perineum C) A hole in the uterus D) An injury to the cervix
- 66. 2. Which of the following is NOT a risk factor of developing an obstetrical fistula A) Being a young first time mother B) Being over age 35 at the time of delivery (advanced maternal age) C) Having (untrained) family members as birth attendants D) Poor nutritional status
- 67. 3. What is a rectovaginal fistula? A) A hole connecting the bladder to the vagina B) A hole connecting the vagina to the uterus C) A hole connecting the rectum to the vagina D) Any hole on the rear wall of the vagina
- 68. 4. Most common cause of VVF in india is: A) Obstructed labour B) Gynaec surgery C) Radiation D) Trauma
- 69. 5. Postpartum VVF is best repaired after: A. 6 weeks B. 8 weeks C. 3 months D. 6 months
- 70. 6. Mrs A, 48yrs had hysterectomy. On seventh day, she devoloped fever, burning micturition & continous dribbling of urine. She can also pass urine voluntarily. The diagnosis is, A. V V F B. Ureterovaginal fistula C. Stress incontinence D. Urge incontinence
- 71. 7.Most useful preoperative investigation for VVF is: A. Three swab test B. Cystoscopy C. Ultrasound D. Urine culture
- 72. 8. If RVF is present in high up(upper part ) preliminary treatment should be: A. Colostomy B. Colporraphy C. Primary repair D. Anterior resection
- 73. ANSWERS 1. A 2. D 3. C 4. A 5. C 6. B 7. B 8. A