Call Girls Frazer Town Just Call 7001305949 Top Class Call Girl Service Avail...
Sarcoma Treatment Algorithms
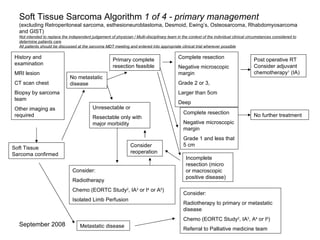
1. Soft Tissue Sarcoma Algorithm 1 of 4 - primary management (excluding Retroperitoneal sarcoma, esthesioneuroblastoma, Desmoid, Ewing’s, Osteosarcoma, Rhabdomyosarcoma and GIST) Not intended to replace the independent judgement of physician / Multi-disciplinary team in the context of the individual clinical circumstances considered to determine patients care All patients should be discussed at the sarcoma MDT meeting and entered into appropriate clinical trial wherever possible History and examination MRI lesion CT scan chest Biopsy by sarcoma team Other imaging as required Soft Tissue Sarcoma confirmed No metastatic disease Metastatic disease Primary complete resection feasible Unresectable or Resectable only with major morbidity Complete resection Negative microscopic margin Grade 2 or 3, Larger than 5cm Deep Complete resection Negative microscopic margin Grade 1 and less that 5 cm Incomplete resection (micro or macroscopic positive disease) Consider reoperation Post operative RT Consider adjuvant chemotherapy 1 (IA) No further treatment Consider: Radiotherapy Chemo (EORTC Study 2 , IA 3 or I 4 or A 5 ) Isolated Limb Perfusion Consider: Radiotherapy to primary or metastatic disease Chemo (EORTC Study 2 , IA 3 , A 4 or I 5 ) Referral to Palliative medicine team
2. Soft Tissue Sarcoma Algorithm 2 of 4 – relapsed disease management (excluding Desmoid, Ewing’s, Osteosarcoma, Rhabdomyosarcoma and GIST) Not intended to replace the independent judgement of physician / Multi-disciplinary team in the context of the individual clinical circumstances considered to determine patients care Patients should entered into appropriate clinical trial wherever possible Local relapse suspected Discuss at MDT meeting Surgery if possible Consider Radiotherapy or Isolated Limb Perfusion Consider other options Isolated local relapse Systemic relapse suspected History and examination CT chest MRI local area Consider imaging nodal drainage region Image any suspicious areas History and examination CT chest Image any suspicious areas Systemic relapse confirmed Solitary site, local therapy possible (consider time interval) Surgery, radiofrequency ablation, radiotherapy Multiple sites or not amenable to local therapy Consider: Chemotherapy (1 st , 2 nd line, phase I or II, other) Palliative medicine referral Radiotharapy Discuss possible further treatment options
3. Soft Tissue Sarcoma Algorithm 3 of 4 – follow up protocol (excluding Desmoid, Ewing’s, Osteosarcoma, Rhabdomyosarcoma and GIST) Not intended to replace the independent judgement of physician / Multi-disciplinary team in the context of the individual clinical circumstances considered to determine patients care All patients should be discussed at the sarcoma MDT meeting and entered into appropriate clinical trial wherever possible History and examination at each visit Follow up may be alternated with surgeons Baseline end of treatment scan of region (MRI or CT) If region difficult to examine clinically – regular imaging required CXR at each visit until 5 years , see table Abnormal primary site Abnormal CXR Clinical suspicion Obtain appropriate imaging of local site, chest and any other suspicious areas Discuss at MDT Further imaging (PET) or biopsy may be required Annual, no CXR Annual, no CXR >10 Annual, no CXR Annual, ?CXR 5-10 Annual 6 monthly 4 6 monthly 3 monthly 3 6 monthly 3 monthly 2 3 monthly 2 monthly 1 Low Grade Clinic visit, clinical examination and CXR High Grade (and intermediate grade) Clinic visit, clinical examination and CXR Year
4.
5. Bone Tumour Algorithm 1 of 2 – primary disease management Not intended to replace the independent judgement of physician / Multi-disciplinary team in the context of the individual clinical circumstances considered to determine patients care All patients should be discussed at the sarcoma MDT meeting and entered into appropriate clinical trial wherever possible Chondrosarcoma Osteosarcoma Ewing’s Sarcoma Primary surgical resection Radiotherapy may be indicated Chemotherapy considered if high grade History and examination Plain X ray lesion MRI lesion CT scan chest Biopsy by sarcoma team Other imaging as required (bone scan) Biochemistry (U&E, LFT, LDH,bone profile) & FBC Diagnosis confirmed No diagnosis Other - specific Further discussion at MDT meeting Further biopsy or resection if possible Neoadjuvant chemotherapy, surgery, further chemotherapy according to EURAMOS (<40yrs) or EUROBOSS (>40yrs) trial protocols Neoadjuvant chemotherapy, surgery, further chemotherapy according to EUROEWING99 trial protocol (<50yrs) Treat according to most appropriate protocol after discussion at MDT
6. Bone Tumour Algorithm 2 of 2 – further management Not intended to replace the independent judgement of physician / Multi-disciplinary team in the context of the individual clinical circumstances considered to determine patients care All patients should be discussed at the sarcoma MDT meeting and entered into appropriate clinical trial wherever possible Local relapse alone Systemic relapse Discuss local management (surgery or RT or other) and timing when other treatment modalities also used Consider systemic therapy Consider palliative care input Image relapse site Image / investigate for other metastases Discuss at MDT if appropriate Consider systemic therapy Consider palliative care input Consider RT or other local therapy to troublesome areas Follow up as for soft tissue sarcoma Trials may have additional requirements
7. GIST - Primary Presentation 1 of 3 Not intended to replace the independent judgement of physician / Multi-disciplinary team in the context of the individual clinical circumstances considered to determine patients care Evaluation Primary Treatment Adjuvant Treatment & Follow-up Note: If available clinical trials should be considered the preferred option for eligible patients Metastatic or unresectable (as determined by surgeon) Localised/ resectable Resect MDT & pathology review CT at 3 months post surgery Pathology review and confirmatory CD 117/c-kit (& /or CD 34) status Consider patient for inclusion in appropriate trials, Three-monthly clinic visits for three years then six-monthly for two years then annual CT (AP) and CXR every six months for three years then annually for a further two years Indefinite clinical review consult appropriate MDT Risk Stratification 1 Low risk Very low risk Clinical presentation and MDT discussion Baseline imaging CT (& /or MRI) (PET if available) High risk Imatinib 400 mg o.d. 2 (see page 2) Follow-up: CT 3 monthly (see page 2) resect if possible Intermediate risk Nil No further scans Primary care follow up Indefinite clinical review Nil Six-monthly for one year then annual One CT (AP) and CXR at 12 months from baseline CT Indefinite clinical review Consider patient for inclusion in appropriate trials, Four-monthly clinic visits for two years then six-monthly for two years then annual CT (AP) and CXR at nine months from baseline then yearly for four years Indefinite clinical review Not a GIST GIST >10 Any size Any >10cm <5 >5cm High risk <5 5-10cm 6-10 <5cm Intermediate risk <5 2-5cm Low risk <5 <2cm Very low risk Mitotic Count (50 cells) Size Risk Stratification 1
8. GIST - Management of Recurrent or Metastatic 2 of 3 Not intended to replace the independent judgement of physician / Multi-disciplinary team in the context of the individual clinical circumstances considered to determine patients care Resect if becomes operable Clinical presentation and MDT discussion Metastatic or Unresectable recurrence (as determined by surgeon) Consider patient for inclusion in appropriate trials e.g. tyrosine kinase inhibitors Response assessments CT at 3 monthly intervals Operable Recurrence Evaluation Baseline imaging CT (& /or MRI) (PET if available) Imatinib 400 mg o.d. 2 ◊ Primary Treatment Assessments & Follow-up PR, CR, SD PD Confirm PD with specialist radiology review – consider PET Localised Multi-focal Escalate dose of Imatinib to 800 mg/day, if tolerable 3 MDT Discussion ? Candidate for surgery and/or RFA of focal progression and continue Imatinib Continue Imatinib 400 mg o.d. Response assessments CT at 3 monthly intervals Resect Pathology review and confirmatory CD 117/c-kit (& /or CD 34) status ◊ See weekly for first month (longer if significant LFT derangement or anticoagulated with warfarin) See monthly for two months, then two-monthly if responding and tolerating treatment well for the first year After one year on Imatinib three or four monthly visits Bloods FBC, U&E, LFTs should be performed at each visit Note: If available clinical trials should be considered the preferred option for eligible patients