

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Sepsis & Septic Shock
Similar to Sepsis & Septic Shock (20)
More from Imhotep Virtual Medical School
More from Imhotep Virtual Medical School (20)
Recently uploaded
Recently uploaded (20)
Sepsis & Septic Shock
- 1. Prepared and presented by Marc Imhotep Cray, M.D.
- 2. Marc Imhotep Cray, M.D. Shock Capsule 2 Shock is a clinical condition characterized by a fast pulse rate (usually > 100 beats/min) and a low blood pressure (systolic blood pressure usually < 100 mmHg) Common types of shock are hypovolemic (low blood volume, e.g. in hemorrhage), cardiogenic (heart pump failure, e.g. in myocardial infarction) septic (severe infection) See: Systems-based Pathophysiologic High Yield Cases-Case 15, Pg. 22. Less common types are anaphylactic (type I hypersensitivity reaction, e.g. penicillin allergy) neurogenic (loss of sympathetic vasomotor tone, e.g. spinal cord injury)
- 3. Marc Imhotep Cray, M.D. Etiology of Circulatory Shock 3 Cardiogenic Shock Myocardial infarction Cardiomyopathy Valvular heart disease Ventricular rupture Congenital heart defects Papillary muscle rupture Obstructive Shock Pulmonary embolism Cardiac tamponade Tension pneumothorax Dissecting aortic aneurysm Hypovolemic Shock Acute hemorrhage Dehydration from vomiting, diarrhea Overuse of diuretics Burns Pancreatitis Distributive Shock Anaphylaxis Neurotrauma Spinal cord trauma Spinal anesthesia Sepsis View Full Presentation: Pathology and Pathophysiology of Shock
- 4. Marc Imhotep Cray, M.D. Stages of Shock 4 Shock is a progressive disorder that leads to death if underlying causes are not corrected Exact mechanisms of sepsis-related death are still unclear; aside from increased lymphocyte and enterocyte apoptosis, cellular necrosis is minimal • Death typically follows the failure of multiple organs usually offer no morphological clues to explain their dysfunction King EG, Bauzá GJ, Mella JR, Remick DG. Pathophysiologic mechanisms in septic shock. Lab Invest. 2014;94(1):4-12. For hypovolemic and cardiogenic shock pathways leading to a patient’s demise are reasonably well understood tissue ischemia, acute tubular necrosis, lactic acidosis severe cellular and tissue injury cardiopulmonary arrest Unless insult is massive and rapidly lethal (e.g., exsanguination from a ruptured aortic aneurysm), shock tends to evolve through three general (albeit somewhat artificial) stages…
- 5. Marc Imhotep Cray, M.D. The 3 Stages of Shock 5 These stages have been documented most clearly in hypovolemic shock but are common to other forms as well: Stage 1 An initial nonprogressive stage during which reflex compensatory mechanisms are activated and vital organ perfusion is maintained Stage 2 A progressive stage characterized by tissue hypoperfusion and onset of worsening circulatory and metabolic derangement, including lactic acidosis Stage 3 An irreversible stage in which cellular and tissue injury is so severe that even if hemodynamic defects are corrected, survival is not possible
- 6. Marc Imhotep Cray, M.D. Comparison of Clinical Findings In Different Types of Shock 6 Copstead LC, Banksia JL. Pathophysiology, 5th Ed. St. Louis, Missouri: Saunders-Elsevier, 2013.
- 7. 7 Sepsis, Organ Dysfunction and Septic Shock: Definitions Sepsis: life-threatening organ dysfunction due to dysregulated host response to infection Organ dysfunction: an acute change in total Sequential Organ Failure Assessment (SOFA) score of 2 points or greater secondary to the infection cause Septic shock: Occurs in a subset of patients with sepsis and comprises of an underlying circulatory and cellular/metabolic abnormality that is associated with increased mortality persisting hypotension requiring vasopressors to maintain a mean arterial pressure of 65 mm Hg or higher and a serum lactate level greater than 2 mmol/L (18 mg/dL) despite adequate volume resuscitation New 2016 definition, also called Sepsis-3, eliminates requirement for presence of systemic inflammatory response syndrome (SIRS) to define sepsis, and it removed severe sepsis definition. What was previously called severe sepsis is now the new definition of sepsis. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA.
- 8. 8 Septicemia Capsule: Septicemia arises through escape of bacteria from a focus of infection such as an abscess Septicemia is more likely to occur in: people with an immunodeficiency disorder, cancer, or diabetes mellitus those who take immunosuppressant drugs, and drug addicts who inject Symptoms include a fever, chills, rapid breathing, headache, and clouding of consciousness Sufferer may go into life-threatening septic shock Treatment Glucose and/or saline are given by intravenous infusion, and antibiotics by bolus injection or IV infusion Surgery may be necessary to remove original infection If treatment is given before septic shock develops, prognosis is good
- 9. Marc Imhotep Cray, M.D. Sepsis & Septic Shock 9 Epidemiology Sepsis is a leading cause of morbidity and mortality in United States, with an estimated incidence rate of 300 cases per 100,000 population and a case fatality rate of 20–50% Medical costs of sepsis in U.S. > $17 billion Rates of sepsis continue to rise secondary to medical advances widespread use of indwelling intravascular catheters, increased implantation of prosthetic material (e.g., cardiac valves and artificial joints), and administration of immunosuppressive drugs and chemotherapeutic agents These interventions serve to increase risk of infect. & subsequent sepsis
- 10. Marc Imhotep Cray, M.D. Sepsis & Septic Shock (2) 10 Sepsis is a continuum of conditions, from infection & bacteremia to sepsis & septic shock Sepsis is life-threatening organ dysfunction caused by a dysregulated immune response to infection • Critical care experts have developed a severity score, called Sequential (Sepsis-related) Organ Failure Assessment (SOFA) score, to predict which patients are at highest risk of dying of sepsis o The score is calculated 24 hours after admission to the ICU and every 48 hours thereafter Septic shock (“Sepsis-3” definition ) includes pts who, despite fluid resuscitation, require vasopressor support and exhibit signs of organ dysfunction (SOFA score ≥2) have a predicted mortality of 40%
- 11. Marc Imhotep Cray, M.D. Sepsis & Septic Shock (2) 11 Another commonly used term is Systemic inflammatory response syndrome ( SIRS ) is a nonspecific inflammatory state that may be seen w infection as well as w noninfectious states (e.g. pancreatitis, pulmonary embolism, and myocardial infarction) Leukopenia and hypothermia, included in SIRS case definition, are predictors of a poor prognosis when associated w sepsis NB: Four SIRS criteria are 1) tachycardia (heart rate >90 beats/min); 2) tachypnea (respiratory rate >20 breaths/min); 3) fever or hypothermia (temperature >38 or <36 °C), and ; 4) leukocytosis, leukopenia, or bandemia (white blood cells >1,200/mm3, <4,000/mm3 or bandemia ≥10%)
- 12. Marc Imhotep Cray, M.D. 12 Hammer GD & McPhee SJ (Eds.). Pathophysiology of Disease: An Introduction to Clinical Medicine, 7th Ed. New York, NY: McGraw-Hill Education, 2014. Clinical definition of sepsis (Prior to 2016)
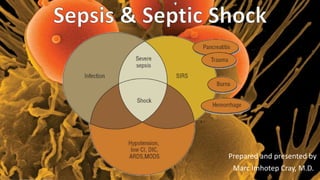
- 13. Marc Imhotep Cray, M.D. Sepsis & Septic Shock 13 Relationship of infection, systemic inflammatory response syndrome (SIRS), sepsis, severe sepsis, and septic shock Abbreviations: ARDS, acute respiratory distress syndrome CI, cardiac index DIC, disseminated intravascular coagulation MODS, multiple-organ dysfunction syndrome Dipiro JT et al, editors: Pharmacotherapy: A Pathophysiologic Approach, 8th Ed. New York: McGraw-Hill, 2011.
- 14. Marc Imhotep Cray, M.D. Sepsis & Septic Shock (5) 14 Etiology Although evidence of infection is a diagnostic criterion for sepsis only 28% of patients w sepsis have bacteremia, and only 10% will have primary bacteremia, defined as positive blood cultures w/o an obvious source of bacterial seeding Common sites of infection among pts. w sepsis syndrome (in decreasing order of frequency) include respiratory tract genitourinary tract abdominal sources (gall bladder, colon) device-related infections, and wound or soft tissue infections
- 15. Marc Imhotep Cray, M.D. Sepsis & Septic Shock (6) 15 Etiology cont. Bacteriology of sepsis: Gram-negative bacteria ( Enterobacteriaceae & Pseudomonas ) , previously most common cause of sepsis, have been supplanted by gram-positive organisms now cause more than 50% of cases o Staphylococci are most common bacteria cultured from bloodstream, b/c of an increase in prevalence of chronic indwelling venous access devices and implanted prosthetic material
- 16. Marc Imhotep Cray, M.D. Pathogenic sequence of events in septic shock 16 Activation of macrophages by endotoxin and other proteins leads to release of inflammatory mediators and immune modulation resulting in host tissue damage and, in some cases, death Hammer GD & McPhee SJ (Eds). Pathophysiology of Disease: An Introduction to Clinical Medicine, 8th Ed. New York, NY: McGraw-Hill Education, 2018.
- 17. 17 Pathophysiology of septic shock Copstead LC, Banksia JL. Pathophysiology, 5th Ed. St. Louis, Missouri: Saunders-Elsevier, 2013.
- 18. Marc Imhotep Cray, M.D. Sepsis & Septic Shock 18 Signs and Symptoms Associated with Sepsis Early Sepsis Fever or hypothermia Rigors, chills Tachycardia Tachypnea Nausea, vomiting Hyperglycemia Oliguria Myalgias Lethargy, malaise Proteinuria Hypoxia Leukocytosis Hyperbilirubinemia Late Sepsis Lactic acidosis Oliguria Leukopenia DIC Myocardial depression Pulmonary edema Hypotension (shock) Hypoglycemia Azotemia Thrombocytopenia ARDS Gl hemorrhage Coma Clinical manifestations of sepsis: Those related to systemic response to infections (tachycardia, tachypnea, alterations in temp. & WBC count) and Those related to specific organ system dysfunction (cardiovascular, respiratory, renal, hepatic, and hematologic abnormalities)
- 19. Marc Imhotep Cray, M.D. Important to identify any potential source of infection 19 Localizing Sn & Sx referable to organ systems may provide useful clues to etiology of sepsis and are as follows: Head and neck infections – Severe headache, neck stiffness, altered mental status, earache, sore throat, sinus pain/tenderness, cervical/submandibular lymphadenopathy Chest and pulmonary infections – Cough (especially if productive), pleuritic chest pain, dyspnea, dullness on percussion, bronchial breath sounds, localized rales, any evidence of consolidation Cardiac infections – Any new murmur, especially in patients with a history of injection or IV drug use
- 20. Marc Imhotep Cray, M.D. Source of infection (2) 20 Abdominal and gastrointestinal (GI) infections – Diarrhea, abdominal pain, abdominal distention, guarding or rebound tenderness, rectal tenderness or swelling Pelvic and genitourinary (GU) infections – Pelvic or flank pain, adnexal tenderness or masses, vaginal or urethral discharge, dysuria, frequency, urgency Bone and soft-tissue infections – Localized limb pain or tenderness, focal erythema, edema, swollen joint, crepitus in necrotizing infections, joint effusions Skin infections – Petechiae, purpura, erythema, ulceration, bullous formation, fluctuance
- 21. Marc Imhotep Cray, M.D. Investigative Images of Septic Shock Cases Source: Kalil, A. Septic Shock. Medscape. Updated: Jan 2019.
- 22. Marc Imhotep Cray, M.D. Strawberry tongue in a child with staphylococcal toxic shock syndrome. Drage, LE. Life-threatening rashes: dermatologic signs of four infectious diseases. Mayo Clin Proc. 1999;74:68-72.
- 23. Marc Imhotep Cray, M.D. Venn diagram showing the overlap of infection, bacteremia, sepsis, systemic inflammatory response syndrome (SIRS), and multiorgan dysfunction. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 24. Marc Imhotep Cray, M.D. A 26-year-old woman developed rapidly progressive shock associated with purpura and signs of meningitis. Her blood culture results confirmed the presence of Neisseria meningitidis. The skin manifestation seen in this image is characteristic of severe meningococcal infection and is called purpura fulminans. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 25. Marc Imhotep Cray, M.D. Gram stain of blood showing the presence of Neisseria meningitidis. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 26. Marc Imhotep Cray, M.D. Acute respiratory distress syndrome (ARDS), commonly observed in septic shock as a part of multiorgan failure syndrome, results in pathologically diffuse alveolar damage (DAD). This photomicrograph shows early stage (exudative stage) DAD. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 27. Marc Imhotep Cray, M.D. Photomicrograph showing delayed stage (proliferative or organizing stage) of diffuse alveolar damage (DAD). Proliferation of type II pneumocytes has occurred; hyaline membranes as well as collagen and fibroblasts are present. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 28. Marc Imhotep Cray, M.D. Acute respiratory distress syndrome (ARDS) in a patient who developed septic shock secondary to toxic shock syndrome. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 29. Marc Imhotep Cray, M.D. Bilateral airspace disease and acute respiratory failure in a patient with gram-negative septic shock. The source of the sepsis was urosepsis. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 30. Marc Imhotep Cray, M.D. A 45-year-old woman was admitted to the intensive care unit with septic shock secondary to spontaneous biliary peritonitis. She subsequently developed acute respiratory distress syndrome (ARDS) and multiorgan failure. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 31. Marc Imhotep Cray, M.D. An 8-year-old boy developed septic shock secondary to Blastomycosis pneumonia. Fungal infections are rare causes of septic shock. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 32. Marc Imhotep Cray, M.D. Soft-tissue infection secondary to group A streptococci, leading to toxic shock syndrome. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 33. Marc Imhotep Cray, M.D. Necrotizing cellulitis of toxic shock syndrome. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 34. Marc Imhotep Cray, M.D. Necrosis of the little toe of the right foot and cellulitis of the foot secondary to group A streptococcal infection. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 35. Marc Imhotep Cray, M.D. Group A streptococci cause beta hemolysis on blood agar. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 36. Marc Imhotep Cray, M.D. Gram stain of blood showing group A streptococci that was isolated from a patient who developed toxic shock syndrome. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 37. Marc Imhotep Cray, M.D. A 46-year-old man presented with nonnecrotizing cellulitis and streptococcal toxic shock syndrome. The leg was incised to exclude underlying necrotizing infection. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 38. Marc Imhotep Cray, M.D. A 46-year-old man presented with nonnecrotizing cellulitis and streptococcal toxic shock syndrome (same patient as in previous image). This patient also had streptococcal pharyngitis. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 39. Marc Imhotep Cray, M.D. A 46-year-old man presented with nonnecrotizing cellulitis and streptococcal toxic shock syndrome (same patient as in previous image). The patient had diffuse erythroderma, a characteristic feature of the syndrome. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 40. Marc Imhotep Cray, M.D. A 46-year-old man presented with nonnecrotizing cellulitis and streptococcal toxic shock syndrome (same patient as in previous image). The patient had diffuse erythroderma, a characteristic feature of the syndrome. He improved with antibiotics and intravenous gammaglobulin therapy. Several days later, a characteristic desquamation of the skin occurred over his palms and soles. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 41. Marc Imhotep Cray, M.D. Progression of soft-tissue swelling to vesicle or bullous formation is an ominous sign and suggests streptococcal shock syndrome. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 42. Marc Imhotep Cray, M.D. Extensive debridement of necrotizing fasciitis of the hand. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 43. Marc Imhotep Cray, M.D. Healing of the hand after aggressive surgical debridement of necrotizing fasciitis (same patient as in previous image). Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. https://emedicine.medscape.com/article/168402-overview
- 44. Marc Imhotep Cray, M.D. Septic Shock: KEY POINTS 44 Septic shock results from a severe systemic inflammatory response to infection • Gram-negative bacteria, gram-positive bacteria, and fungal infections are common causes of septic shock • In gram-negative shock, endotoxins in bacterial cell walls stimulate massive immune system activation • Septic shock from any organism is characterized by release of large numbers of immune mediators (e.g., cytokines) resulting in widespread inflammation • The clotting cascade, complement system, and kinin system are activated as part of immune response
- 45. Marc Imhotep Cray, M.D. Septic Shock: KEY POINTS 45 Widespread inflammation leads to profound peripheral vasodilation with hypotension, maldistribution of blood flow with cellular hypoxia, and increased capillary permeability with edema formation Initially, septic shock is characterized by abnormally high cardiac output resulting from immune-mediated vasodilation and sympathetic activation of the heart • Patient is usually febrile, pink, and warm. Even though cardiac output is high, cellular hypoxia is present because of maldistribution of blood low • Reduced cellular oxygen utilization is manifested as a high SvO2 Therapy for septic shock is aimed at improving distribution of blood flow and managing infection with antibiotics. Administration of fluid and drugs to increase cardiac and vascular performance is done to improve distribution of blood low
- 46. 46 THE END
- 47. Marc Imhotep Cray, M.D. Sources and further study: 47 Copstead LC, Banksia JL. Pathophysiology, 5th Ed. St. Louis, Missouri: Saunders-Elsevier, 2013. Dipiro JT et al, eds. Pharmacotherapy: A Pathophysiologic Approach, 8th Ed. New York: McGraw-Hill, 2011. Kalil, A. Septic Shock. Medscape. Updated: Jan 2019. Kishiyama JL. Ch. 3 Disorders of the Immune System, Pgs. 31-59 and Bloch KC. Ch. 4 Infectious Diseases, Pgs. 61-87 In: Hammer GD and McPhee eds. JS. Pathophysiology of Disease : An Introduction to Clinical Medicine, 7th Ed. New York: McGraw-Hill Education, 2014’ Johnson AG et al. Bacterial Diseases. In: Microbiology and immunology. 4th Ed. Baltimore: Lippincott Williams & Wilkins, 2010. eLearning (Cloud) Infectious Disease Pathology Microbial biology & Immune System Textbooks: Ryan KJ and Ray CG Eds. Sherris Medical Microbiology, 5th Ed. New York: McGraw-Hill, 2010. Carroll KC etal. Jawetz, Melnick, & Adelberg’s Medical Microbiology 27th Ed. New York: McGraw-Hill, 2016.