
Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Lipid metabolism and Hypolipidemics
Ähnlich wie Lipid metabolism and Hypolipidemics (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Lipid metabolism and Hypolipidemics
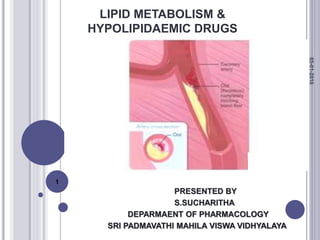
- 1. LIPID METABOLISM & HYPOLIPIDAEMIC DRUGS PRESENTED BY S.SUCHARITHA DEPARMAENT OF PHARMACOLOGY SRI PADMAVATHI MAHILA VISWA VIDHYALAYA 05-01-2016 1
- 2. CONTENTS INTRODUCTION LIPIDS LIPOPROTEINS LIPOPROTEIN CLASSIFICATION LIPID METABOLISM EXOGENOUS PATHWAY ENDOGENOUS PATHWAY ATHEROGENESIS DRUG THERAPY SUMMARY REFERENCES 05-01-2016 2
- 3. Cardiovascular and cerebrovascular ischemic diseases has becoming a leading cause of morbidity and mortality A major cause for the development of IHD is high cholesterol & related dyslipidemia Disorders of the metabolism of lipoproteins, including lipoprotein over production and deficiency are classified as DYSLIPIDEMIA These may manifest in one or more of the following ways: Elevated total cholesterol levels Elevated LDL cholesterol levels Elevated triglycerides levels Decreased HDL cholesterol levels INTRODUCTION 05-01-2016 3
- 4. LIPIDS I)SIMPLE LIPIDS ( esters of fatty acids and alcohol) 1. Saturated fatty acids- which have sizeable effect of raising blood cholesterol Eg : lauric and palmitic acid 2. Mono unsaturated fatty acids- helps in lowering of LDL & VLDL Eg :oleic acid & palmitoleic acid 3. Poly unsaturated fatty acids- they have hypolipidemic effect Eg : linoleic acid & arachidonic acid 4. Trans fatty acids- they are harmful as they raises LDL & lowers HDL Eg : elaidic acid 05-01-2016 4
- 5. II)COMPOUND LIPIDS (also esters of fatty acids but have other groups in their structure) Eg: sulpholipids and phospholipids III)NEUTRAL LIPIDS ( they are non polar lipids) Eg: cholesterol, triglycerides, cholesteryl esters 05-01-2016 5
- 6. LIPOPROTEINS Lipids by definition are insoluble in water. In order to transport lipids such as fatty acids, triacylglycerol, steroids and fat soluble vitamins in the blood plasma, a carrier protein is required. The bulk of the body’s lipids (cholesterol, phospholipids and triacylglycerol), are transported in the plasma by large complexes called lipoproteins. These lipoproteins consist of a core of hydrophobic lipids surrounded by a shell of phosphatidyl glycerol and proteins. The protein components of lipoproteins solubilise the hydrophobic lipids and contain the cell targeting signals. 05-01-2016 6
- 8. CLASSIFICATION OF LIPOPROTEINS Lipoproteins can be classified in three ways- 1) Based on density- They are separated by Ultracentrifugation. Depending upon the floatation constant (Sf), Five major groups of lipoproteins have been identified that are important physiologically and in clinical diagnosis. (i) Chylomicrons, derived from intestinal absorption of triacylglycerol and other lipids; Density is generally less than 0.95 while the mean diameter lies between 100- 500 nm. (ii) Very low density lipoproteins (VLDL), derived from the liver for the export of triacylglycerol; density lies between 0.95- 1.006 and the mean diameter lies between 30-80 nm. 05-01-2016 8
- 9. (iii) Intermediate density lipoproteins (IDL) are derived from the catabolism of VLDL,with a density ranging intermediate between Very low density and Low density lipoproteins i.e. ranging between 1.006-1.019 and the mean diameter ranges between 25-50nm. iv) Low-density lipoproteins (LDL), representing a final stage in the catabolism of VLDL; density lies between 1.019-1.063 and mean diameter lies between 18-28 nm (iv) High-density lipoproteins (HDL), involved in cholesterol transport and also in VLDL and chylomicron metabolism. Density ranges between 1.063-1.121 and the mean diameter varies between 5-15 nm. 05-01-2016 9
- 10. Lipoproteins with high lipid content will have low density, larger size and so float on centrifugation. Those with high protein content sediment easily, have compact size and have a high density. 05-01-2016 10
- 11. 2) Based on electrophoretic mobilities Lipoproteins may be separated according to their electrophoretic properties into - α, pre β, β, and broad beta lipoproteins. HDL are -α , VLDL pre- β, LDL-β , and IDL are broad beta lipoproteins. 05-01-2016 11
- 12. 3)Based on nature of Apo- protein content Apoproteins are the transport proteins that bind to lipids to form lipoproteins. Apo lipoproteins also serve as enzyme cofactors, receptor ligands, and lipid transfer carriers that regulate the metabolism of lipoproteins and their uptake in tissues. They have specific structural domains that are recognized by cell receptors. All of the apoproteins have amphipathic α-helixes with the hydrophobic side chains facing the lipid interior of the lipoprotein and the hydrophilic residues interacting with the polar head groups of the phospholipids or interacting with the aqueous solvent. 05-01-2016 12
- 13. FUNCTIONS OF APO PROTEINS (1) They can form part of the structure of the lipoprotein, e.g. Apo B, structural component of VLDL and Chylomicrons. (2) They are enzyme cofactors, e.g. C-II for lipoprotein lipase, A-I for lecithin cholesterol acyltransferase(LCAT), or enzyme inhibitors, Eg: Apo A-II and Apo C-III for lipoprotein lipase, Apo C-I for cholesteryl ester transfer protein. (3) They act as ligands for interaction with lipoprotein receptors in tissues, e.g. Apo B-100 and Apo E for the LDL receptor, Apo A-I for the HDL receptor. 05-01-2016 13
- 14. Apo protein Lipoprotein classes Function A-I Chylomicrons, HDL Activates LCAT A-II Chylomicrons, HDL Inhibits LCAT, enhances hepatic lipase activity. A-IV Chylomicrons Unknown function B-100 VLDL, IDL, HDL Necessary for binding to cell receptors, LPLs. B-48 Chylomicrons Necessary for binding to cell receptors, LPLs. C-I Chylomicrons, VLDL, HDL Cofactor for LCAT C-II Chylomicrons, VLDL, HDL Activates LPL C-III Chylomicrons, VLDL,HDL Regulates LPL D HDL Essential for LCAT activity and Cholesteryl ester transfer. E ALL Binds to specific cell receptors. CHARACTERISTIC DIFFERENCE OF LIPOPROTEINS 05-01-2016 14
- 15. 05-01-2016 15
- 16. LIPOPROTEIN METABOLISM Each class of lipoproteins has a specific role in lipid transport and there are different pathways, which are distinguished by the main Apoprotein (apo-B48, apo-B100, apo-A1), respectively that are ligand for key receptor, they are LIPOPROTEIN METABOLISM EXOGENOUS PATHWAY ENDOGENOUS PATHWAY Apo-B100 Guided pathway a. Apo-A1 guided pathway 05-01-2016 16
- 17. 05-01-2016 17
- 19. EXOGENOUS PATHWAY In intestine the triglycerides & cholesterol is incorporated into the core of chylomicrons Chylomicrons are acted upon by the enzyme lipoprotein lipase . Reaction with lipoprotein lipase results in the loss of approximately 90% of the triacylglycerol of chylomicrons and in the loss of Apo C (which returns to HDL) but not Apo E, which is retained. The resulting chylomicron remnant is about half the diameter of the parent chylomicron and is relatively enriched in cholesterol and cholesteryl esters because of the loss of triacylglycerol Chylomicron remnants are taken up by the liver by receptor-mediated endocytosis, and the cholesteryl esters and triacylglycerols are hydrolyzed and metabolized. for the synthesis of VLDL.
- 20. 05-01-2016 20
- 21. In intestine the triglycerides & cholesterol is incorporated into the core of chylomicrons CMs are transported into circulation where apo-c is transferred to it from HDL In capillary endothelium Apo-C activates LPL which hydrolyses CMs results in the loss of approximately 90% of the triacylglycerol of chylomicrons and in the loss of apo C (which returns to HDL) After hydrolysis the result CMR which contain CE>TG gets detached from capillary endothelium Chylomicron remnants are taken up by the liver by receptor- mediated endocytosis, and the cholesteryl esters and triacylglycerols are hydrolyzed and cholesterol get liberated EXOGENOUS PATHWAY
- 22. Uptake is mediated by apo E . Hepatic lipase has a dual role: (1) it acts as a ligand to facilitate remnant uptake and (2) it hydrolyzes remnant triacylglycerol and phospholipids Finally in this pathway Fatty acids formed from triglycerides are delivered to fats and muscles Cholesterol serves as a component for synthesis of: •Cell membrane •Bile acids •Steroids •Also enters endogenous pathway
- 24. ENDOGENOUS PATHWAY The endogenous lipid transport system conveys lipid from liver to peripheral tissues & back to the liver. It can be separated into two subsystems The atherogenic Apo-B100 lipoprotein governed system(VLDL,IDL&LDL) The antiatherogenic Apo-A1 governed lipoprotein system(HDL) 05-01-2016 24
- 25. In liver the core lipids are packed together with Apo-B100 & phospholipids into VLDL Then these are secreted into plasma where Apo-CI,CII,CIII&E are added to nascent VLDL from circulating HDL The TGs in VLDL are hydrolysed by capillary LPL present on luminal surface of blood vessel of various tissues forming FREE FATTY ACIDS VLDL after hydrolysis converted to VLDL remnants If this VLDL further contains TGs then it is called as IDL IDL further enters into liver through endocytosis via LDL receptors which recogise Apo-E & hydrolyses the IDL to LDL with help of HL APO-B100 LIPOPROTEIN GOVERNED SYSTEM 05-01-2016 25
- 27. ENDOCYTOSIS OF LDL 1. LDLs bind to specific cell receptors located on the plasma membrane of target cells. 2. The LDL receptor is a glycoprotein which contains a domain with negatively charged residues. 3. This LDL binding domain has electrostatic interactions with the positively charged arginine and lysine residues of apo-B100. 4. The LDL receptors migrate to areas of the plasma membrane specialized for endocytosis called coated pits. 5. They are called coated pits because of the clathrin protein coat on the cytoplasmic side of the membrane.
- 28. 6. Once the LDL binds to the receptor, the clathrin proteins promote endocytosis. 7. Once the vesicle is inside of the cell, the clathrin spontaneously dissociates from the endosomal vesicle. 8. The pH of the vesicle is lowered such that LDL dissociates from the receptor. 9. The LDL receptors are recycled to the cell surface. 10. The vesicle fuses with a lysosome which then degrades the lipoprotein to its primary components, fatty acids, glycerol, cholesterol and amino acids. The cholesterol is incorporated into the intracellular cholesterol pool which is used for membrane or steroid synthesis.
- 29. HYPERCHOLESTEROLEMIA Familial hypercholesterolemia is a genetic disease caused by a defective LDL receptor. There are five classes of mutations that have been identified with the disease. 1. The receptor is not synthesized at all. 2. The receptor is not transported to the surface of the cell. 3. The receptor fails to bind LDL. 4. The receptor fails to cluster in the clathrin coated pits. 5. The receptor may fail to release LDL in the endosome. 05-01-2016 29
- 30. Deficiency of the LDL receptor results in increased concentration of LDL. Having one gene that produces an abnormal LDL receptor is called heterozygous familial hypercholesterolemia 05-01-2016 30
- 31. APO-A1 CONTAINING LIPOPROTEIN SYSTEM Nascent HDL is synthesised by intestine & liver which contain mainly Apo-A1 & phospholipids HDL3, generated from discoidal HDL by the action of LCAT, accepts cholesterol from the tissues via the SR-B1 and the cholesterol is then esterified by LCAT, increasing the size of the particles to form the less dense HDL2. HDL3 is then reformed, either after selective delivery of cholesteryl ester to the liver via the SR-B1(REVERSE TRANSPORT PATHWAY) or by hydrolysis of HDL2 phospholipids and triacylglycerol by hepatic lipase. This interchange of HDL2 and HDL3 is called the HDL cycle. Free apo A-I is released by these processes and forms pre -HDL after associating with a minimum amount of phospholipids and cholesterol 05-01-2016 31
- 32. A second important mechanism for reverse cholesterol transport involves the ATP-binding cassette transporter A1 (ABCA1). ABCA1 preferentially transfer cholesterol from cells to poorly lipidated particles such as pre -HDL or Apo A-1, which are then converted to HDL3 & then to HDL2 via discoidal HDL These cholesterol rich HDL2 containing CE are exchanged for triglycerides with VLDL,IDL,LDL & CMR with the help of CETP The result is the cholesterol enrichment of Apo-B & triglycerides enrichment of HDL2 TGs of HDL2 converts back to HDL3 by hydrolysis HDL2 is catabolised by liver HDL2 can return to liver by SR-B1 receptors which removes CH converting it back to HDL2 05-01-2016 32
- 33. FUNCTIONS OF HDL Scavenging action- HDL scavenges extra cholesterol from peripheral tissues by reverse cholesterol transport HDL with the help of Apo E competes with LDL for binding sites on the membranes and prevents internalization of LDL cholesterol in the smooth cells of the arterial walls HDL contributes its Apo C and E to nascent VLDL and chylomicrons for receptor mediated endocytosis HDL stimulated prostacyclin synthesis by the endothelial cells, which prevent thrombus formation HDL also helps in the removal of macrophages from the arterial walls . 05-01-2016 33
- 34. ATHEROGENESIS Atheroma is a focal disease of the intima of large and medium-sized arteries. Lesions evolve over decades, during most of which time they are clinically silent, the occurrence of symptoms signalling advanced disease. Presymptomatic lesions are often difficult to detect non-invasively, although ultrasound is useful in relatively static and superficial arteries (e.g. the carotids), and associated changes such as reduced aortic compliance and arterial calcium deposition can be detected by measuring, respectively, aortic pulse wave velocity and coronary artery calcification. 05-01-2016 34
- 36. ATHEROGENESIS endothelial dysfunction, altered PGI2, NO biosynthesis Injury of endothelium, expression of adhesion molecules, migration of monocytes transport of LDL particles to blood vessels, generation of free radicals by endothelium that oxidizes LDL results in lipid peroxidation oxLDL taken up by macrophages via SR-B1 receptors forming FOAM CELLS that releases pro inflammatory cytokines FATTY STREAK Cholesterol mobilised from artery wall & transported to plasma in the form of HDL Activated platelets, macrophages & endothelial cells cause proliferation of smooth muscle and results in ATHEROMATOUS PLAQUE PLAQUE RUPTURE ,THROMBOSIS ,STABILISATION OF PLAQUE 05-01-2016 36
- 38. DRUG THERAPY IN ATHEROGENESIS CLASSIFICATION 1 . HMG-CoA reductase inhibitors (Statins): Lovastatin Simvastatin Pravastatin Atorvastatin Rosuvastatin Pitvastatin 2. Bile acid sequestrants (Resins): Cholestyramine Colestipol 3. Activate lipoprotein lipase (Fibric acid derivatives): Clofibrate Gemfibrozil Bezafibrate Fenofibrate 4. Inhibit lipolysis and triglyceride synthesis: Nicotinic acid 5.Antioxidant: Probucol 6. Sterol absorbtion inhibitors: Ezetimibe 7.Others: Gugulipid. 05-01-2016 38
- 39. HMG CO-A REDUCTASE INHIBITORS OR STATINS DRUGS Lovastatin Rosuvastatin Atorvastatin Pitvastatin Simvastatin Pravastatin ADVERSE EFFECTS Gastro intestinal disturbance Muscle pain, Headache, Insomnia Rashes, Rarely myopathy & angio-oedema USES First time of drug both familial & secondary hyperlipidemia as in DIABETES MILLETUS. Useful in lowering morbidity & mortality in patients with coronary heart disease HMG CO-A MEVALONIC ACID CHOLESTROL STATINS HMG CO A REDUCTASE 05-01-2016 39
- 40. FIBRATES/ FIBRIC ACID DERIVATIVES DRUGS Clofibrate Gemfibrozil Bezafibrate Fenofibrate OTHER ACTIONS They also increases HDL They also increases oxidation of fatty acids in liver & decreases lipolysis in adipose tissue ADVERSE EFFECTS GI disturbances Skin rashes, Headache, Myositis Muscle cramps, Blurred vision Rhabdomyolysis FIBRATES LPL SYNTHESIS Degradation of VLDL TGs LDL Activates PPAR α receptors 05-01-2016 40
- 41. BILE ACID BINDING RESINS DRUGS Cholestyramine Colestipol USES Used in patients with raised LDL levels Used along with lovastatin or nicotinic acid BAB RESINS (+vely charged) Bind to –vely charged bile acids in intestine Prevent absorption of cholesterol Fall in plasma cholesterol LDL levels 05-01-2016 41
- 42. INHIBITORS OF LIPOPROTEIN & TRIGLYCERIDES SYNTHESIS DRUGS Nicotinic acid ADVERSE EFFECTS Cutaneous vasodilatation Feeling of warmth mediated by PGs Dyspepsia, Dryness & Pigmentation USES Used in hypertriglyceridemia with low HDL level Nicotinic acid Inhibit TG synthesis in the liver HDL Production of VLDL LDL 05-01-2016 42
- 43. STEROID ABSORPTION INHIBITORS Adverse effects diarrhoea, abdominal pain or headache rash and angio-oedema USES As an addition to a statin when response has been inadequate (ezetimibe). For hypercholesterolemia when a statin is contraindicated. Uses unrelated to atherogenesis, including: Pruritis in patients with partial biliary obstruction (bile acid-binding protein) Bile acid diarrhoea. Ezetimibe & its metabolites Concentrated in the brush border of the small intestine Inhibit a specific transport protein NPC1L1 Cholesterol absorption LDL 05-01-2016 43
- 44. Antioxidant Probucol decreases LDL & increases HDL It is generally not preferred o Miscellaneous Gugulipid decreases the plasma cholesterol & TGs Omega 3 Fatty Acids (Fish Oils)-The most widely used n-3 PUFAs for the treatment of hyperlipidemia are the two active molecules in fish oil: Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA). 05-01-2016 44
- 45. INVESTIGATIONAL Investigational classes of hypolipidemic agents: CETP inhibitors (cholesteryl ester transfer protein), 1 candidate is in trials. It is expected that these drugs will mainly increase HDL while lowering LDL; Squalene synthase inhibitor; ApoA-1 Milano Succinobucol (AGI-1067), a novel antioxidant, failed a phase 3 trial Apo protein-B inhibitor Mipomersen (approved by the FDA in 2013 homozygous familial hypercholesterolemia). PCSK9 Monoclonal antibody inhibitors 05-01-2016 45
- 46. SUMMARY Lipid s are fats that are either absorbed from food or synthesized by the liver. Lipids are transported by a special protein called lipoprotein & gets metabolised by 2 major pathways i.e., exogenous & endogenous pathway Any alteration in the lipid metabolism will leads to the one of the following disorder Hyper cholesterolemia Hyper triglyceridemia Chylomicron retention disease LIPIDS EXOGENOUS ENDOGENOUS VLDL IDL LDL HDL store energy in adipocytes & muscle cells cell membranes, steroids, bile acids and signalling molecules. LIPOPROTEI N ATHEROSCELEROSIS 05-01-2016 46
- 47. REFERENCES RANG AND DALES PHARMACOLOGY: 8TH ADDITION. PRINCIPLES OF PHARMACOLOGY BY H.L.SHARMA & K.K.SHARMA ESSENTIALS OF MEDICAL PHARMACALOGY BY K.D.TRIPATI 6TH EDITION A CASE ORIENTED APPROACH TOWARDS BIOCHEMISTRY BY: NAMRATA CHHABRA, SAHIL CHHABRA REVIEW OF LIPOPROTEINS BY BRYANT MILES 05-01-2016 47
- 48. 05-01-2016 48
- 49. 05-01-2016 49