Ewing's sarcoma
•Als PPTX, PDF herunterladen•
15 gefällt mir•5,391 views

Ewings Sarcoma.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Ewing's sarcoma
Ähnlich wie Ewing's sarcoma (20)
Mehr von Sreekanth Nallam
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Ewing's sarcoma
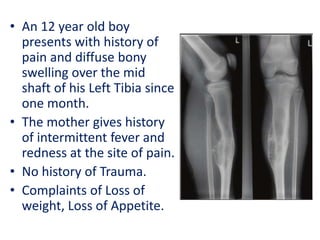
- 1. • An 12 year old boy presents with history of pain and diffuse bony swelling over the mid shaft of his Left Tibia since one month. • The mother gives history of intermittent fever and redness at the site of pain. • No history of Trauma. • Complaints of Loss of weight, Loss of Appetite.
- 2. Differential Diagnosis •Osteomyelitis •Osteoid osteoma •Eosinophilic Granuloma •Ewing’s tumour •Osteosarcoma
- 3. Osteomyelitis Osteoid osteoma Ewing’s tumour Osteosarcoma Eosinophilic Granuloma Presentation Pain, Redness, Fever, Weakness. Dull pain, Limping, swelling. Pain, Swelling, Pathological fracture. Pain, swelling, worse at night Pain Age All ages 5-25 years 8-20 years Bimodal distribution (<25 &>60 yrs) Adolesents/ Young adults. Sex Males Males(3:1) Males(1.5- 2:1) Males Equal Duration Short/Long Long Short Short short Benign/ Malignant Infective origin Commonest benign Second most Bone cancer in childern. Most common Bone cancer in childern. Benign bone lesion soild periosteal reaction Site Usually at metaphysis Diaphysis Diaphysis - Femur, tibia, flat bone Metaphysis: Femur, tibia (knee) Skull, ribs, Femur. (Metaphysis) Others No h/o trauma Pain relieved with NSAIDs Can have H/O Trauma Most with H/O Trauma H/O fever, Trauma.
- 5. • Ewing’s sarcoma is the second most common bone cancer of children, following osteosarcoma. • The median age at presentation is 14 years (usually 8–25 years) • Boys are affected more than girls (1.5–2:1)
- 6. • American Pathologist • Suffered from OM at the age of 14yrs. • Confined to bed for 2 yrs. • Served as Prof of Pathology for 33 yrs at Cornell Univ. New York. • Died of bladder cancer at 76yrs. • Described in 1921 as an undifferentiated tumor involving the diaphysis of long bones that is radiation sensitive (in contrast to osteosarcoma). James Stephen Ewing (1866-1943)
- 7. At Presentation: • Pain (>90%) • Swelling or mass (65%) • Limitation in movement (25%) • Neurologic changes (15% overall, though 50% in central tumors) • Pathologic fracture (15%) • Fever (10%) • Approximately 25% have overt metastases at presentation.
- 10. • Usually show an area of bone destruction which is predominantly in the mid-diaphysis. • New bone formation may extend along the shaft and sometimes appears as fusiform layers of bone around the lesion – ‘onion-peel’ effect. • Often the tumour extends into the surrounding tissues, with radiating streaks of ossification (‘sunray’ appearance) and reactive periosteal bone at the proximal and distal margins (Codman’s triangle).
- 12. The definitive diagnosis is based on • Histomorphologic findings • Immunohistochemistry • Molecular pathology HISTOMORPHOLOGICAL FINDINGS: • Neuroectodermal tissue is the embryonic tissue of origin for EWS and it is derived from primordial BM mesenchymal stem cells. • Ewing's sarcoma is a small-blue-round-cell tumors • Have a clear cytoplasm on H&E staining, due to glycogen. • The presence of the glycogen can be demonstrated with • Positive PAS staining and • Negative PAS diastase staining. • Differential for small round blue cell tumors (mnemonic LEMONS): Lymphoma, Ewing’s, Medulloblastoma, Other (rhabdomyosarcoma, pineoblastoma, ependymoblastoma, etc.), Neuroblastoma, Small cell carcinoma.
- 16. • The characteristic immunostain is CD99, which diffusely marks the cell membrane. (CD99 is not specific for Ewing's sarcoma) • The most common translocation, present in about 90% of Ewing sarcoma cases, is t(11;22)(q24;q12) • Generates an aberrant transcription factor through fusion of the EWSR1 gene with the FLI1 gene.[FLI1(11): EWS(22)] • Other minor translocations include: • t(21;22), c-Myc proto-oncogene(chromosome 21) and EWS gene(chromosome 22) in 10% of cases. • t(7;22)
- 17. • Ewing’s family of tumors includes • Ewing’s sarcoma (bone 87%), • Extraosseous Ewing’s sarcoma (8%), • Peripheral PNET (5%), and • Askin’s tumor (PNET of chest wall). • Markers that differentiate EWS: 1. Vimentin 2. HBA-71 3. β2-microglobulin 4. ↑c-myc (vs. n-myc in NB) • PNET and EWS have similar translocations and are both CD99 (MIC2)+ and vimentin+. • PNET is NSE+, S100+, more differentiated, and has more neuroendocrine features. • EWS is NSE−, S100 variable, and Homer Wright rosettes+.
- 18. At presentation • 75-80% of patients present with localized disease. • 25% of EWS pts present with mets. Lung (25%–40%) ≥ Bone/BM (∼25%) and LNs (<10%). • Bone Marrow micromets are seen in 25% (localized) & 40% (lung mets) 5-yr OS: • Localised disease is 60-70% • Metastatic EWS: 1. Lung mets: ∼35% 2. Bone/BM mets: ∼25% 3. Lung + bone/BM mets: ∼15% (Paulussen M et al., Ann Oncol 2009)
- 19. Poor prognosis in EWS • Male gender • Age >15 yrs (>17 yrs in some) • Pelvic/axial Site or rib origin • Size (>8 cm per St. Jude or >100 cc per CESS- 81 [Cooperative Ewing Sarcoma Studies]) • Stage (presence/absence of metastatic Dz is strongest prognostic factor) • ↑LDH • Poor response to chemo (>10% viable tumor) • No surgery
- 21. Chemotherapy • IESS-1 (JCO 1990): – Nonrandomized comparison of 342 patients with localized disease treated with VAC + D vs. VAC vs. VAC + prophylactic bilateral whole lung RT plus noncontrolled local intervention. – 5-year RFS was best with VAC + D (60%) vs. VAC (24%) vs. VAC + RT (44%). – VACA is superior to VAC or VAC + BPR. VAC + bilateral pulmonary RT is superior to VAC. No improvement between treatment modalities was noted for pelvic cases. • IESS-2 (JCO 1991): – 214 patients with localized nonpelvic primaries randomized to high-dose, intermittent VAC + D vs. moderate dose continuous VAC + D. – Local treatment was surgery ± postoperative RT or RT alone (whole bone to 45 Gy with primary boost to 55 Gy). – High-dose VAC + D improved OS (63 → 77%); no difference in OS for local control modalities. – High dose intermittent VACA is superior to the IESS-I regimen, even for pelvic tumors. OS actually superior to nonpelvic pts in IESS-I. – Take home: Intermittent VACA is standard of care. • IESS-3/INT 0091 (NEJM 2003): – 518 patients with localized or metastatic disease randomized to VDCA vs. VDCA alternating with IE. – Local treatment was given at week 9–15 with RT, surgery, or both. – Adding IE improved 5-year OS (61 → 72%) for localized disease, but not for metastatic disease (25%). – VACA+IE superior to VACA for OS and localized disease, but no benefit in metastatic disease. – Take home: high dose, intermittent VACA+IE is standard of care.
- 22. • IESS-IV tested dose intensification of VAdriaC+IE • AEWS0031 tested interval compression of VAdriaC+IE These showed that VAdriaC+IE q2wks was superior and forms the current standard of care in the definitive setting. • COG protocol AEWS0031 a randomized trial for patients with newly diagnosed localized Ewing sarcoma. • This trial sought to intensify therapy not by dose escalation, but by decreasing the interval between chemotherapy cycles (interval compression). • Patients randomized to receive VDC/IE cycles alternating every 3 weeks vs 2 weeks. • 5-year event-free survival (73% versus 65% for patients randomized to the standard arm). • This trial established interval compressed VDC/IE as a new standard approach for patients with localized Ewing sarcoma.
- 23. • VAC/IE (vincristine + doxorubicin [Adriamycin] + cyclophosphamide alternating with ifosfamide + etoposide) • Alternating VAC and IE cycles. • Repeat each cycle every 3 weeks for 17 cycles. VAC cycles • Day 1: Vincristine 2mg/m2 (max 2mg) IV + doxorubicin 75mg/m2 IV bolus + cyclophosphamide 1,200mg/m2 IV. – Dactinomycin can be substituted for doxorubicin if there are concerns regarding cardiotoxicity – Dactinomycin 1.25mg/m2 IV can be substituted for doxorubicin when a total doxorubicin dose of 375mg/m2 is reached. IE cycles • Days 1–5: Ifosfamide 1,800mg/m2 IV + mesna + etoposide 100mg/m2 IV.
- 25. Surgery: • For local control, Surgery preferred unless poor functional results are anticipated. • Resection provides pathologic information post-chemotherapy, avoids second malignancy and late effects of RT. • Resection without reconstruction can be done in small bones such as rib, clavicle, proximal fibula, distal scapula, metatarsals, metacarpals, and small iliac wing or pubic bone lesions. • Results are typically very good for these “dispensable bones.” • Large lesions may require allograft or endoprosthetic reconstructions. • Metastatic setting: – Limited pulmonary metastases – Palliation at primary site • Nodal dissection is not routinely indicated. LOCAL THERAPY
- 26. • Adequate surgical margins in EWS Per COG protocol AEWS0031(Womer RB et al., JCO 2012) – >1 cm for bone – >0.5 cm for Sdft Tissue – >0.20 cm for fascia • Sg is preferred – Expendable bones are involved – If there is a pathologic fracture • 3 indications for adj RT after Sg in EWS: – +Margin – Tumor spill – >10% viable tumor after induction chemo (poor chemo response).
- 27. Radiation: • RT potentially indicated pre-op, post-op, or definitively for the primary tumor and for treatment of pulmonary and skeletal metastases. • Indications for postoperative RT – Close margins (<1 cm) – Poor histologic response (<90% necrosis) – Tumor spill. • Preoperative RT considered when close/positive margins are expected. • Treat pre-chemo volume due to high rate of local failure if limited to post-chemo volume. • Involved field rather than whole bone is sufficient. • Hyperfractionation does not improve outcomes, but may improve fracture rate, range of motion, and muscle atrophy. • Adjuvant RT starts at the time of consolidation CHT (week 14). • VC-IE CHT is given during RT (doxorubicin held during RT).
- 28. No randomized trials have directly compared RT to surgery for LC of Ewing’s sarcoma. • CESS 86 (JCO 2001): – 177 patients with localized Ewing’s treated with chemotherapy – Nonrandomized local control arms of • Surgery alone • Surgery plus 45 Gy RT • Definitive RT of 60 Gy (randomized to qd vs. b.i.d.). – RT used 5 cm proximal/distal margins and 2 cm lateral/deep margins. – 5-year OS was 69% with no differences in OS or RFS according to local therapy. – Local control was 100% for surgery, 95% for surgery plus RT, and 86% for RT alone (no difference for qd vs. b.i.d. RT).
- 29. • POG-8346 (Donaldson SS et al., IJROBP 1998) – Osseous EWS pts after induction chemo rcvd definitive RT for local therapy randomized to • Whole bone RT (39.6 Gy → 55.8 Gy boost to GTV +2 cm) vs. • Involved-field RT (GTV + 2 cm to 55.8 Gy) • All pts then rcvd maintenance chemo. • The RT Tx techniques had similar 5-yr EFS (∼41%) and LC (∼53%).
- 30. CESS-81 and -86 and EICESS 92 (European Intergroup CESS) • Schuck et al. (IJROBP 2003) • Performed a secondary analysis of 1,085 pts • Compared PreOP RT vs. PORT vs. Definitive RT • Local Failure – Similar b/t preop and postop RT (5.3% vs. 7.5%) but – Significantly worse in the definitive RT arm (26%) • Criticism: There was a strong negative selection bias against the definitive RT cohort. • There was no difference in LF b/t RT alone and Sg + post-RT if only partial resection was achieved. • In CESS-81, Disease free survival after 41 months for patients with – Tumor volume <100 ml was 75% – Tumor volume greater than or equal to 100 ml was 10% • Preop RT may improve LC if unresectable.
- 31. • Talleur (IJROBP 2016): –St. Judes phase II trial of 45 EWS patients –Randomised to 55.8 vs. 64.8 Gy based on tumor size <8 vs. ≥8 cm, respectively. –All patients treated with 1 cm margins on gross tumor. –LF rate 4.4% at 10 year.
- 32. Chest wall Ewings Sarcoma (Rib primary & Askin’s tumor) • More commonly seen in females. • Preoperative CHT – Improves negative margins (50% vs. 77%) – Decreased need for post-op RT (5-yr EFS 56%) • Schuck A et al. retrospectively reviewed 138 pts with localized CW EWS treated in CESS-86 and EICESS 92. (IJROBP 2002) – 42 pts rcv hemithorax RT. – If <14 yo, then 15 Gy; otherwise, 20 Gy at 1.5 Gy/fx or 1.25 Gy bid. – All RT pts rcv a boost to the primary site of 45–60 Gy. – 7-yr EFS trended in its favor (63% vs. 46%). – Improvements in EFS appeared to be d/t reductions in pulmonary mets. – A major criticism of this study is that the RT group had sup chemo.
- 33. METASTATIC DISEASE • If patient has Lung Mets: • Chemotherapy → WLI or surgical resection (if <5 mets). • EICESS secondary analyses: Paulussen et al. (a) isolated pulmonary mets or (b) combined lung + bone/BM mets – Treated +/– WLI as part of a series of protocols from the EICESS. – WLI was associated with improved EFS in both subgroups. (Ann Oncol 1998) • St. Jude’s retrospective study: Rodriguez-Galindo et al. – EWS pts with isolated pulmonary recurrence. – Pts who rcvd WLI had improved 5-yr postrecurrence survival (30% vs. 17%). (Cancer 2002)
- 34. • The WLI dose in EWS depends on age: – If <14 yo, then 15 Gy (1.5 Gy/fx) – If ≥14 yo, then 18 Gy (mostly in European protocols, but US protocols still use 15 Gy). The field borders used in WLI for EWS. • Superior–Inferior: 1 cm above 1st rib to L2 (Block PA kidney at 7.5 Gy) • Lateral: 1 cm lat rib cage.
- 35. RADIATION DOSES • Radiation fields customized depending on primary site • MRI is recommended for treatment planning in all cases • Definitive RT for bone tumors with no soft-tissue involvement: – Prechemotherapy GTV plus a 2 cm margin to 55.8 Gy. • Definitive RT for bone tumors with a soft-tissue component: – Prechemotherapy GTV plus a 2 cm margin to 45 Gy boost to 55.8 Gy to the initial bony GTV + postchemotherapy soft-tissue extent with a minimal margin. • For postoperative RT – Pretreatment GTV plus a 2 cm margin to 45 Gy boost -Postoperative microscopic/tumor spill + 2 cm margin to 50.4 Gy -Gross residual disease + 2 cm margin to 55.8 Gy. • 45 Gy for vertebral body involvement b/c of SC tolerance.
- 36. • LN positive—resected: Nodal Bed-50.4 Gy in 1.8 Gy/fx • LN positive—unresected: Nodal level: 45 Gy, Gross node: 55.8 Gy in 1.8 Gy/fx • Malignant ascites/diffuse peritoneal involvement: – Whole abdomen RT: 25 Gy in 1.5 Gy/ fx • Lung metastases: Whole lung RT: 15 Gy in 1.5 Gy/fx – (if <6 years, then 12 Gy in 1.5 Gy/fx) • Chest wall tumor/pleural nodules/effusion: – Hemithorax RT: 15 Gy in 1.5 Gy/fx – Chest wall tumor: • Prechemo volume +1.5-2cm=30.6 Gy • Postchemo Volume+1.5-2cm=36 Gy in 1.8 Gy/fx – Pleural nodule: • Prechemo volume +1.5-2cm=21.6 Gy • Postchemo Volume+1.5-2cm=36 Gy in 1.8 Gy/fx. AEWS1031 contouring guidelines
- 37. COMPLICATIONS 1) Dermatitis and recall reaction: ADR and dactinomycin A. 2) Cystitis: Cyclophosphamide or ifosfamide or RT cystitis. 3) Abnormal bone and soft-tissue growth and development. – Premature epiphyseal closure: occurs at >20 Gy. – Decreased bone growth can occur at ∼10 Gy. – Limb length discrepancy of 2–6 cm can be managed with a shoe lift. – Consider amputation and prosthesis in the very young as they recover function well.
- 38. 4) Permanent weakening of affected bone. – The highest risk for fracture is within 18 months of RT, during which time patients should avoid contact and high-impact sports. – Factors that influence fracture risk • Total dose, extent of cortical disruption at Dx, younger age, and 2nd bone malignancy in the RT field. 5) Decreased range of motion secondary to soft-tissue and/or joint fibrosis. 6) Lymphedema can be prevented by – Sparing a 1–2-cm strip of skin on the extremity or – Minimize the circumferential RT dose to 20–30 Gy
- 39. 7) Second malignancy • Kuttesch et al. retrospectively reviewed 266 EWS pts treated at St. Jude’s Hospital. • 20-yr cumulative incidence of 2nd malignancies was – 9.2% for any malignancy and – 6.5% for sarcoma • RT dose–response relationship with a 2nd malignancy RR of 40 if RT was >60 Gy and minimal for <48 Gy. (JCO 1996) • Most common second tumor is osteosarcoma.
- 40. Chemotherapy Side effects: – Vincristine (neuropathy, constipation, myalgias, arthralgias, and cholestasis) – Cyclophosphamide (pancytopenia and dose-dependent hemorrhagic cystitis, infertility) – Doxorubicin (myocardial dysfunction and pancytopenia) – Ifosfamide (high incidence of hemorrhagic cystitis requiring use of Mesna and Fanconi syndrome of electrolyte wasting) – Etoposide (pancytopenia, anaphylactic reactions, and second malignancies such as AML).
- 41. FOLLOW-UP • H&P + CXR every 3 months for 2 years. • X-ray primary every 3 months (and/or MRI every 6 months) for 2 years. • After 2 years, may increase follow-up intervals, but should obtain CBC annually.
Hinweis der Redaktion
- Ewing’s sarcoma commonly presents in Lower extremity (femur 15–20%, tibia or fibula 5–10%), Pelvis (20–30%), Upper extremity (humerus 5–10%), Ribs (9–13%), and Spine (6–8%).
- S100 calcium binding protein B Neuron-Specific Enolase
- 75-80% of patients present with localized disease, but 20–25% have gross metastases to the lung, bone, or bone marrow, and nearly all patients have micrometastases at diagnosis, so all patients require chemotherapy.
- dose intensity defined as the amount of drug delivered per unit of time [mg/m²/week].
- Local Failure rate for EWS after definitive RT: 5%–25% Worse with pelvic sites (LF 15%–70%) Worse with large (>8 cm) lesions (LF 20%).
- Cooperative Ewing Sarcoma Study
- In a recent review of RT-induced osteosarcoma, most common primary was Ewing’s (25%), median latency was 8 years. 5-yr OS was 40% overall, with aggressive CHT and surgery 5-yr OS 68% versus chemo alone 17%.